Total Knee Arthroplasty
 Total knee arthroplasty (OAG) is a completely successful surgical procedure, as it offers patients permanent pain relief and restoration of joint mobility. Sophisticated minimally invasive techniques and improved implant design have significantly increased surgery success rates, offering patients a better quality of life.
Total knee arthroplasty (OAG) is a completely successful surgical procedure, as it offers patients permanent pain relief and restoration of joint mobility. Sophisticated minimally invasive techniques and improved implant design have significantly increased surgery success rates, offering patients a better quality of life.
Do I need a total knee arthroplasty (OAG)?

The decision to replace the knee joint involves weighing the expected benefit and the potential risk, if any. Essentially, if the knee has significant wear and tear from arthritis and does not respond to conservative treatment (medications, physiotherapy, injections) then it needs replacement.
The decision is easy if you suffer a lot and can’t walk long distances. Even more so, if you are older. Most people who undergo OAG are over 70 years old. Postponing the operation, if you have severe arthritis, makes the muscles weaker, makes the knee stiffer and deformed, and makes the result less successful. On the other hand, if you are young, you may not yet wish to undergo a major operation. Therefore, the doctor may advise you to change your lifestyle, e.g. with exercise and weight loss. If you are under the age of 50 it is likely that you will need a second OAG operation (“revision”) later in life.
As with the hip, a knee is replaced mainly for the following reasons:
- Pain, which is the most common cause
- Deformation
- Limitation of functionality, e.g. instability, stiffness
- To protect neighboring joints,
It is usually the final and definitive solution when conservative treatment has failed and other surgical treatments are not feasible. The knee with osteoarthritis is classically deformed. It is usually deformed into a curvature, i.e. the knees look outward. Sometimes there can be a deformity in hallux valgus, that is, the knees look inward and are in contact with each other. Hallux valgus is usually more difficult to operate on due to various technical factors. It is also more common in patients with rheumatic diseases, while the torn knee is usually a classic example of osteoarthritis.

What can I expect from an OAG?
More than 90% of OAG lasts more than 15 years. They are just as effective as total hip arthroplasties. However, there are many factors that determine the success of an OAG. People’s expectations vary widely.
Pain after total knee replacement
Most patients have minimal residual pain after the first six months after surgery. But, even those who have, usually see further improvement over a year.
Self-care after total knee replacement
The majority of patients now have minimal difficulty after an OAG:
- to take care of themselves
- to be washed
- carry out their daily needs and activities
- to move
- Do his shopping
- even to play sports
Walking after total knee replacement
The improvement in gait is particularly important and great after surgery. Most patients can walk for as long as they want without pain. Some may need a cane, especially if they have delayed surgery or have been using a cane for a long time. In general, patients are in better physical condition one year after surgery. Usually, it is not easy to kneel after an OAG because the surgical incision is in the middle and front, making it painful to kneel.
Stability and functionality of the joint after total knee arthroplasty
Before total knee arthroplasty, a lack of knee stability is a common symptom. But, it is not at all common after it. Before total arthroplasty, most people cannot go up or down stairsor do it with great difficulty. This improves significantly after total knee arthroplasty. For younger patients, an OAG may not allow them to return to heavy manual labor.
Recovery after a total knee replacement is longer compared to a total hip arthroplasty. Don’t expect your knee to bend completely from the start, particularly if it was stiff enough before surgery. Therefore, you may still have difficulty doing things that need a lot of knee flexion, such as: squatting, kneeling, or deep squatting.
What preparation should the patient do before total knee arthroplasty?
Patients can make various changes to both their lifestyle and at home to help them recover faster from surgery.
Lifestyle changes
- Smoking restriction: Smokers are more vulnerable to respiratory complications during anesthesia, but also to respiratory infections after surgery. This can prolong bedtime, lie down, and delay the patient’s recovery.
- Weight loss: An overweight patient is more difficult to operate on than a thin one, larger detachments are needed which usually involves more bleeding. Overweight patients are also more vulnerable to respiratory complications. Overweight patients should lose as much weight as possible, as even a small weight loss helps. The lighter weight will also subject the post-surgery arthroplasty to lighter loads.
- Medications: Prescription medications for heart, blood pressure, diabetes mellitus, etc. should be taken regularly by the patient. Thus, the patient will remain in good condition before surgery.
- Exercise: Patients should exercise as much as possible. The better their physical condition before surgery, the easier it is to restore them after surgery.
Changes in the house
It also makes sense to prepare the patient for the period after surgery. After surgery, the patient will find it difficult to bend his knee even though he may have undergone an excellent total arthroplasty. Most arthroplasties bend to right angles in the first period after surgery and gradually improve with daily exercise. For this reason, it can be difficult:
- sitting in low seats
- regularly going up and down stairs
- to kneel
- squatting
So higher seats or other aids may be needed to avoid bending over, kneeling, etc.
Preoperative examination
As with other major operations, the patient must be evaluated before surgery. The assessment is done by the anesthesiologist, cardiologist or other specialties if necessary, to make sure that it is in good condition for it. The preoperative examination is performed one to two days before the operation. A complete history is usually taken and various tests are performed, as listed below:
- Blood tests to check hematocrit and parameters, such as sugar, urea, electrolytes, creatinine, etc. Also, blood will need to be taken for cross-referencing. This ensures that there will be blood available in case a transfusion is needed after the operation. However, in the vast majority of cases, you don’t have to.
- Urine is also checked because it is crucial that there is no urinary tract infection at the time of surgery.
- Chest X-rays to check that there is no respiratory infection.
- An electrocardiogram and examination by a cardiologist to check the function of the heart.

What happens in the hospital?
Admission to the hospital is usually made early in the morning of the day of surgery. On the day of admission, you are seen by the nurses, the anesthesiologist and the surgeon and you sign a consent sheet.
How is anesthesia performed for total knee arthroplasty?
A venous catheter will be inserted into you, usually on the back of the hand. Through the venous catheter, drugs for anesthesia and analgesia, as well as antibiotics to prevent infections, will be administered. You will discuss with the anesthesiologist which anesthetic is appropriate for you. Possible options are general anesthesia with which you will sleep and be intubated. However, spinal or epidural anesthesia (regional anesthesia) is more likely to be performed, in which case you will not understand your body from the waist down. These are done by inserting a needle into the lumbar spine of your spine and injecting medication. There is also the possibility, which is the most common practice, for a combination of the above methods, regional anesthesia combined with sedation, so that you do not feel what is happening at the time of surgery.
How is total knee arthroplasty performed?
The operation involves an incision in the anterior part of the knee, the length of which varies depending on the patient’s dimensions and the surgeon’s technique. With minimal intervention techniques (MIS) the length of the incision has been minimized compared to the past. This access allows the surgeon to reveal the arthritic knee, remove the arthritis-worn surfaces and prepare them to accommodate the prostheses. In addition, the placement of artificial grafts is done with or without the use of bone cement.
The success of a total knee replacement and its long-term survival depends on both the stability of the fixation and the correct alignment of the knee joint. Depending on the technique followed by the surgeon, there are different types of alignment, and manufacturers of total knee arthroplasties provide the appropriate tools. These allow the surgeon to place the bone incisions in such a way as to ensure a good alignment. Robotic surgery helps in this exact point, offering greater precision in the placement of prostheses.
Completion of the operation
Total knee arthroplasty lasts about an hour and a half. After the operation is completed, a tube is placed inside the wound in order to drain blood from the knee after the operation for the first 24 hours. The purpose of this is to avoid the large hematoma in and around the knee. Otherwise, its creation causes pain and delay in recovery. During the operation there is no blood loss, because the operation is performed under an ischaemic bandage. More specifically, a plastic femur is placed around the leg, high at thigh level. Much like a blood pressure monitor, it inflates at high pressure and stops blood circulation to the lower limb. As a result, the operation is performed without the loss of blood and with better visibility for the surgeon.
The wound after surgery is sutured with great emphasis on suturing the bursa and quadriceps, because it is of great importance for postoperative recovery. The skin is also sewn up, usually with metal clips and the patient returns to his room after a short stay in resuscitation.
What happens after the operation is completed?
Before returning to your room, spend some time in resuscitation. There you will be given serums for hydration and medications, such as painkillers, antiemetics and others, from the vein. The wound will be covered with gauze and bandages. If spinal or epidural anesthesia was used then you will not feel your legs and pain for a few hours. The use of a urinary catheter is also a common practice, both for practical reasons that have to do with the patient’s mobility, and for reasons of paresis of the bladder from anesthesia.
For the first 24 – 48 hours after surgery, your pain will be checked by medications given to you by the anesthesiologist and by the local injection of drugs into the joint by the surgeon before the completion of the operation. You may have an analgesic injection device into your spine (epidural pump).

Medication will also be used to avoid thrombosis of the leg and, by extension, a possible pulmonary embolism. The most common method of anticoagulant treatment is the use of low molecular weight (HMBB) heparin injections. They are done subcutaneously in the abdomen, around the navel, or on the arm. Alternatively, newer preparations are oral anticoagulants, which have been used successfully in recent years.
When can I leave the hospital?
The usual length of stay in the hospital is 1 to 2 days. During this time you will be able to walk alone out of the room without assistance but with the support of a walker or bacteria. You will be able to go to the toilet with little support for getting up and down from the bed while you will be able to go up and down stairs on your own. So there is usually no reason to stay in the hospital any further unless other medical reasons require it. Sutures are removed two to three weeks after surgery, and usually no changes to the wound are required after discharge from the hospital.
Physiotherapy after total knee replacement
Already on the day of the surgery you will be able to get up in a sitting position on your bed. From the first postoperative day, your physiotherapy and mobilization begins. Walking is relatively easy after an OAG and is achieved from the very first postoperative day. Leg muscle strengthening and knee flexion-extension exercises also start from the first postoperative day.
Postoperatively, you will start exercises under the guidance of a specialized physiotherapist, which are extremely important for the success of the operation. A knee to be functional must fully stretch and bend at least at right angles. Half of this is achieved in the operating room, but the other half is achieved with proper postoperative rehabilitation. A decisive factor is the persistent efforts of the patient himself.
How long does recovery take?
Every patient and every knee is different and so some patients have a faster recovery and some others a slower recovery. This depends primarily on the preoperative condition of the patient and the leg. Thus, patients with a good muscular system and without contraction preoperatively have a faster postoperative recovery. On the contrary, neglected cases are very likely to delay achieving the desired result, but sooner or later it will eventually be achieved.
You will need a “pi” type walker or two crutches for the first period. This period varies from a few days to a month. It is expected that your knee is swollen or even has ecchymosis, i.e. hematomas. In cases of larger swellings or hematomas, recovery may be a little slower, but the end result will be the same. Some patients are very enthusiastic and cause greater swelling by being too active. In this case, the surgeon or physiotherapist will instruct you to limit mobility. The main priority is to nourish the wound safely in the first two weeks.
The first weeks at home
Your activity will be limited for the first two to four weeks after an OAG because your knee will be heavy and you will need support. You will need pain relievers to be able to do your exercises. Ice is very useful for both resolving swelling and pain. You should exercise daily and several times during the day, repeating the exercises shown to you by your physiotherapist and doctor at the hospital. The aim is to achieve the range of motion from full extension to a bend of at least 110°C-120°C. There is no specific restriction on sleeping position after a total knee arthroplasty.
The most important thing to know is that in the first few days after surgery you will probably not be able to take care of yourself, i.e. cook for yourself or others or do other household chores. It is therefore very likely that you will need help from another person in the house, who will be able to do these tasks for you or even help you to go to the bathroom or other activities.
Review and Remediation
The surgeon will want to see you again a month after the surgery. By then you will have logically gotten rid of the bacteria support and you will be able to drive again if you want. If you were using support before surgery, then you probably still need some support during this time. However, it would be good to avoid standing for long hours or lifting weights until the period of three months after surgery. During this time, you have usually already begun to forget the operation you underwent.
Of course, there may be variations in this recovery protocol which depend, as mentioned above, on the age and condition of the patient, but often also on the severity of the surgery. This is because a knee arthroplasty revision, for example, may need a longer recovery period as well as knees that have had significant deformities.
What materials are used for the new joint?
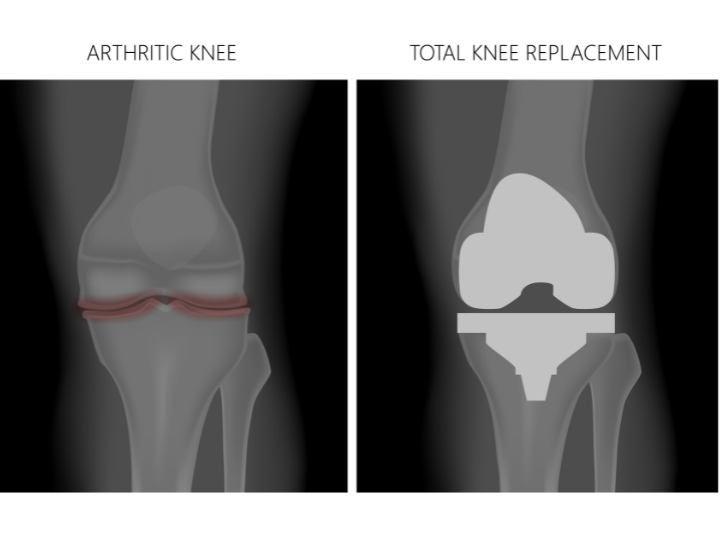
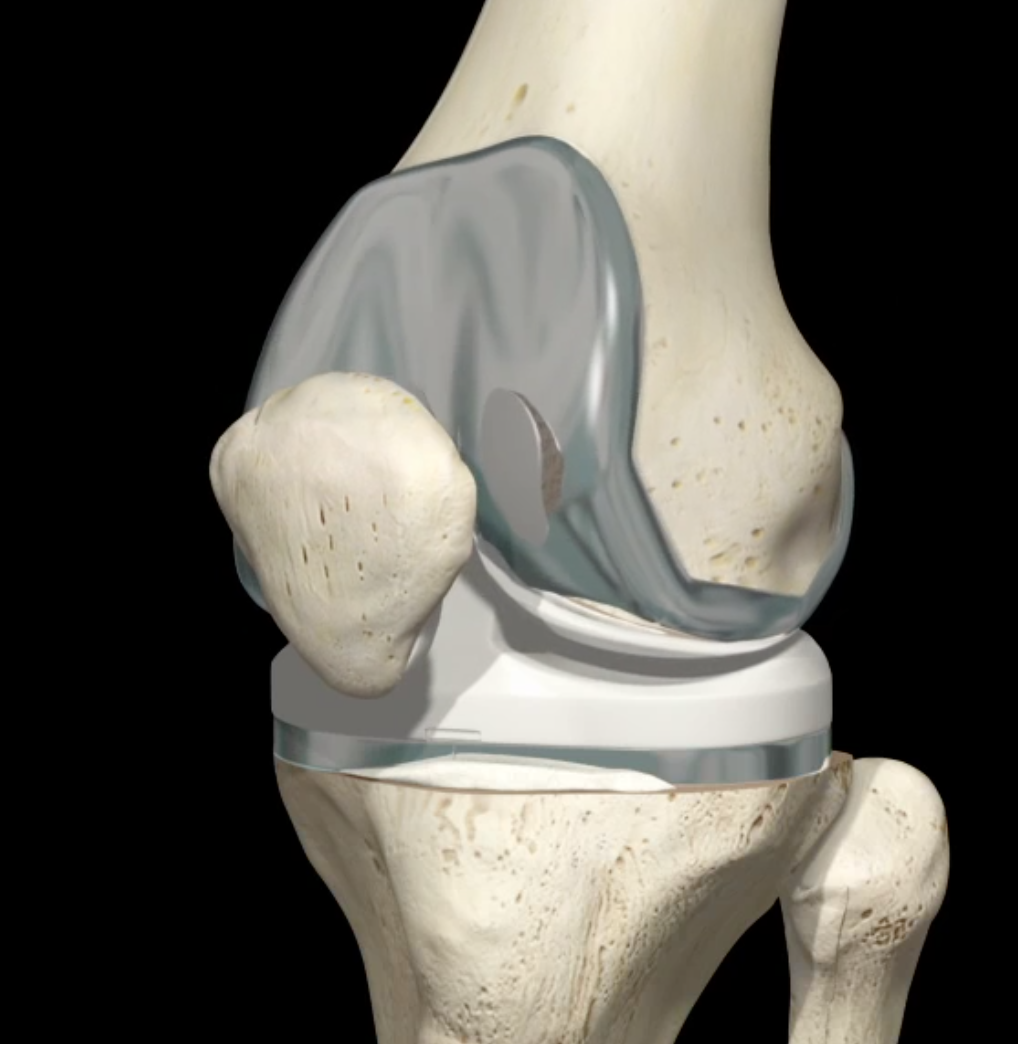
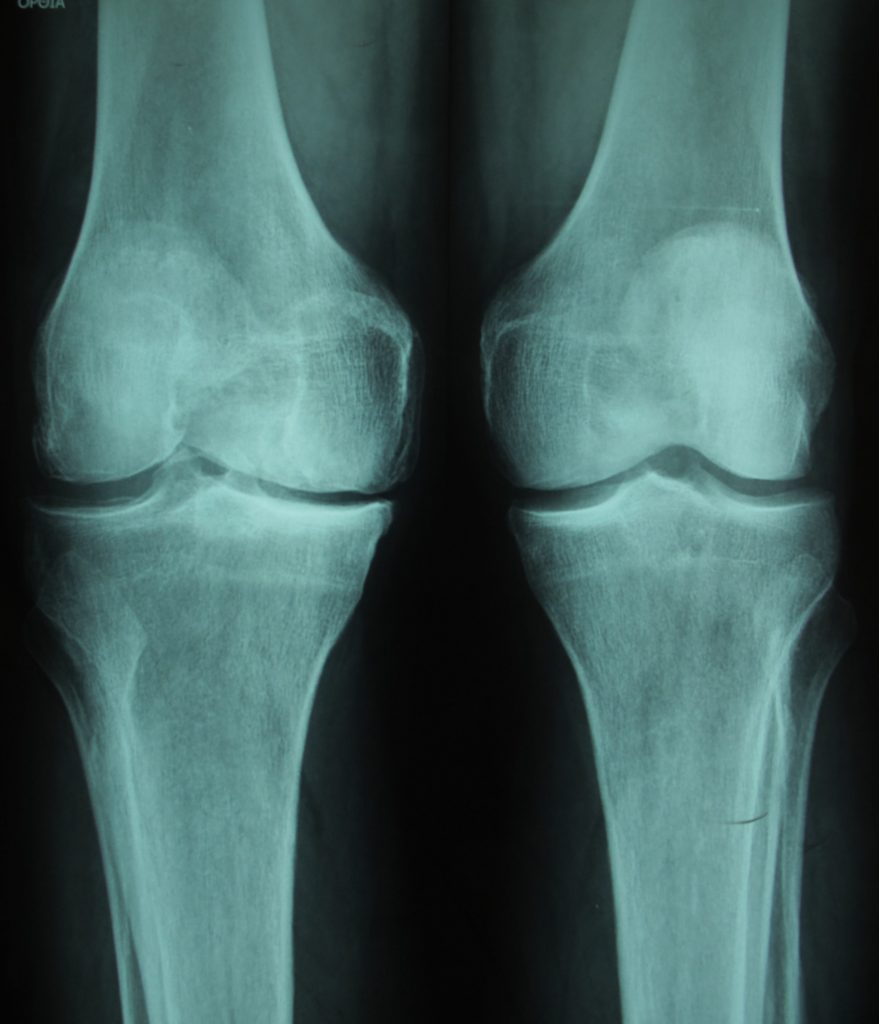
The normal knee gives you the feel of a hinge but actually moves in a much more complex arc. This allows your knee to move rotationally and sideways. The articular cartilage that covers the ends of the femur and tibia allows the bones to move easily against each other. Arthritis destroys this cartilage, causing one bone to rub against the other and cause pain.
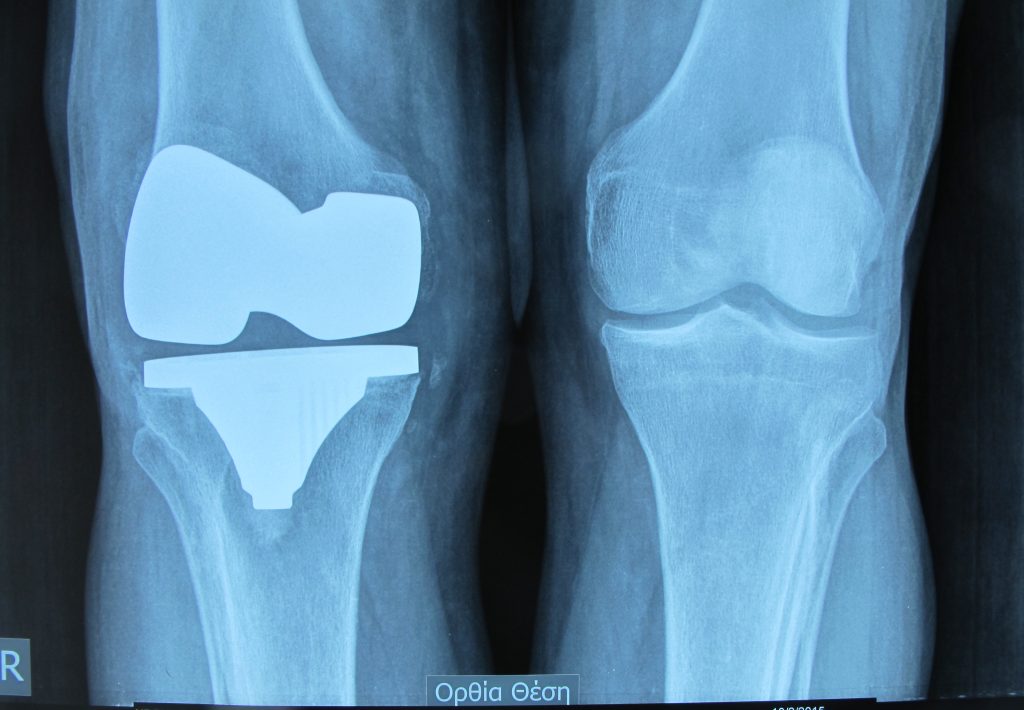
To replace the knee joint, the surgeon carefully removes the cartilage and worn hypochondrial bone and replaces them with metal alloy prostheses. These materials have been used for many years and have been successfully tested with their design constantly improving with the newest materials. The end of the femur is replaced by a convex part of metal with a configuration that resembles the real femur. The upper end of the tibia is replaced by a flat metal segment of the same shape as the real one. Between these two prostheses, a piece of plastic (high molecular weight polyethylene, UHMWP) is placed that binds to the tibia, replaces the cartilage and menisci and prevents metal-to-metal contact. With the new joint, the stability in the knee is given by the shape and design of the prosthesis in combination with the other stabilizing elements (ligaments, muscles, etc.).
What are the two types of knee arthroplasty?
There are two different types of knee replacement depending on the patient’s needs:
- Non-restrictive type arthroplasty: The usual design of an OAG. Both surfaces or partitions, as we call them, are replaced.
- Monocompartmental knee arthroplasty: This is used in cases where only one part of the joint, or one compartment, as it is called, has wear. This operation is less severe, has a faster recovery and is usually, but not exclusively, indicated in younger people with less damage to the joint, as an operation to postpone the heavier total arthroplasty.
Knee replacement during a knee replacement is a controversial issue among surgeons. There is the school (mainly in America) that always chooses to replace it, and the school (mainly in Europe) that never does so. As it is obvious, every practice has its advantages and disadvantages.
Finally, the usual practice for fixing implants is the use of bone cement which provides immediate fixation. Nevertheless, there are designs of total arthroplasty in which fixation is done without the use of bone cement.


Complications
Although complications are not common , unfortunately they do exist, as in any surgery or medical procedure in general. They can be divided into two categories: those that occur as a result of surgery in general (general complications) and those that are specific to total knee arthroplasties (specific complications).
General complications
- Complications from the urinary tract: It is quite common for patients to have difficulty urinating after surgery. Usually, it is the result of lying down, anesthesia, limited mobility and pre-existing problems mainly in men. For this reason, the placement of a urinary catheter is chosen for the first few days.
- Cardiovascular complications: The most common cardiovascular complication is deep vein thrombosis, which, however, in recent years with the rapid mobilization of patients and appropriate preventive anticoagulant treatment is a rare occurrence. Even rarer and consequential to the previous one, is the formation of a clot that can cause a stroke or pulmonary embolism.
- Respiratory complications: These usually occur as a result of anesthesia and lying down. Patients with previous respiratory or heart problems are more prone to these complications.

Specific complications
- Relaxation: In cases of sagging, the grafts need to be revised and changed. Of course, it must be made clear that the rate of relaxation depends to a large extent on the surgeon, the materials and the patient himself. So usually an experienced surgeon who uses the best materials usually has a much lower rate of relaxation than the general population of surgeons.
- Instability: After a total knee arthroplasty, the ligaments may be looser than desired and cause instability in the joint. When it is mild, it is not a problem. Sometimes, however, a new operation may be needed to correct this condition.
- Delayed wound healing: Total knee arthroplasty involves implanting synthetic materials very close to the skin. It is therefore possible that the skin cannot heal properly It is very important that the wound is kept as clean as possible until complete healing takes place. Rarely, a breakdown of the wound can occur. This means that the wound opens up and needs to be rejuvenated and sutured anew.
- Arthroplasty infection which can occur immediately after surgery or many years after it: This will usually be treated with strong antibiotics. Sometimes, a reoperation may be necessary, which will be performed in one or two stages.
- Sensation disorder around the knee: It is normal for patients after knee replacement to lose sensation on the outside of the knee. This is not a functional problem. The nerves that are cut by the surgical incision are not restored and thus a skin hypoesthesia is caused.
Frequently asked questions about total knee replacement
Is my knee still painful?
Rarely, your knee pain does not calm down within the first 3-4 weeks of surgery. If this happens, talk to your doctor, who will diagnose a possible problem and advise you. In the vast majority of cases there is no problem. You may just need rest from exercises or modified analgesic treatment. Swelling and hematomas may also take longer for some people to absorb.
My knee is still stiff
Sometimes, for no apparent reason, the knee becomes very stiff in the first few weeks after surgery. The more you try to exercise your knee, the more stiff and painful it becomes. Consult your doctor. A few days without exercises with simple rest can greatly improve the image.
Can an artificial knee joint be replaced with another?
Yes, it can.
If an OAG wears out (this can usually happen after 15-20 years), then it can be replaced with another arthroplasty. This revision operation is more difficult than the first. The old joint and cement that has been used will be removed and replaced with new ones. Revision of total knee arthroplasty is now a routine operation.
What developments are there?
The developments in OAG have been very important in recent years. There are continuous improvements in the design and manufacture of arthroplasties, but above all major advances in surgical and anesthesiological techniques:
- Optimization of anesthesiological techniques.
- Regulation of postoperative pain with better and newer drug combinations.
- Prevention of postoperative complications such as nausea, thrombosis or constipation, with the use of appropriate preparations.
Thus, the faster return of the operated patient to the previous state and the shorter stay in the hospital have been achieved.
However, the most decisive factor for achieving this is the use of the latest surgical techniques of minimal invasive surgery. By performing joint replacement through smaller surgical incisions, minimizing muscle damage, reducing surgical time, and selecting patients appropriately, we have achieved:
- faster recovery of both the joint and the patient.
- less reliance on support.
- the reduction of postoperative pain.
- faster return to full operations.
Conclusion
Total knee arthroplasty is one of the most successful orthopedic surgeries, with excellent long-term success rates. However, it is important that the replacement of the joint is done by an experienced and qualified Orthopedic Surgeon, as it requires precision and attention to the movements.
Orthopedic Surgeon Anastasios Lilikakis has many years of experience and expertise in knee surgery using all modern surgical techniques. He is the Chairman of the Department of Reconstructive Hip & Knee Surgery of the Hellenic Orthopaedic Society and Director of the Third Orthopaedic Clinic of the Athens Euroclinic. If you have problems with your knee, contact Mr. Lilikakis for early diagnosis and the right choice of treatment method for your case. Contact us immediately to book your appointment.
Πόσο σύντομα μετά την επέμβαση της αρθροπλαστικής γόνατος θα μπορέσω να περπατήσω;
Μετά από μια αρθροπλαστική γόνατος, η κινητοποίηση του ασθενούς ξεκινά συνήθως πολύ νωρίς, εντός των πρώτων ωρών μετά την επέμβαση, υπό την καθοδήγηση φυσικοθεραπευτή. Η άμεση φόρτιση του σκέλους είναι εφικτή στις περισσότερες περιπτώσεις, καθώς τα σύγχρονα υλικά προσφέρουν υψηλή σταθερότητα. Ωστόσο, η ικανότητα για αυτόνομο βάδισμα χωρίς βοηθήματα εξαρτάται από πολλούς παράγοντες, όπως η ηλικία του ασθενούς, η γενική του φυσική κατάσταση, η ποιότητα του μυϊκού συστήματος και η συμμόρφωση στο πρόγραμμα αποκατάστασης. Συνήθως, η βάδιση πραγματοποιείται με πατερίτσες ή «πι» για λίγες ημέρες, ενώ η πλήρης ανεξαρτησία στο βάδισμα επιτυγχάνεται προοδευτικά μέσα σε διάστημα 2-4 εβδομάδων.
Πόσο διάστημα θα παραμείνω στο νοσοκομείο;
Η διάρκεια νοσηλείας μετά από μια αρθροπλαστική γόνατος ποικίλλει, ανάλογα με την τεχνική που εφαρμόζεται, τη γενική κατάσταση υγείας του ασθενούς και την ταχύτητα ανάρρωσης. Στα σύγχρονα πρωτόκολλα ταχείας αποκατάστασης (Fast Track), η παραμονή στο νοσοκομείο μπορεί να περιοριστεί ακόμη και σε 1–2 ημέρες, ενώ σε πιο κλασικές προσεγγίσεις η νοσηλεία κυμαίνεται συνήθως στις 3–5 ημέρες.
Η πρώιμη κινητοποίηση, η αποτελεσματική αναλγησία και η εντατική φυσικοθεραπεία συμβάλλουν στη μείωση του χρόνου νοσηλείας, επιτρέποντας στον ασθενή να επιστρέψει πιο γρήγορα στο οικείο περιβάλλον του με ασφάλεια. Παρά ταύτα, η τελική απόφαση για το εξιτήριο καθορίζεται εξατομικευμένα, βάσει της πορείας ανάρρωσης και της δυνατότητας αυτόνομης βάδισης με ή χωρίς βοήθημα.
Πότε μπορώ να επιστρέψω στη δουλειά μου μετά από την αρθροπλαστική γόνατος;
Η επιστροφή στην εργασία μετά από μια αρθροπλαστική γόνατος αποτελεί σημαντικό στάδιο της αποκατάστασης και διαφοροποιείται ανάλογα με το είδος της απασχόλησής σας και την πορεία ανάρρωσης. Εάν η εργασία είναι καθιστική, όπως σε γραφείο ή σε περιβάλλον χωρίς ιδιαίτερες σωματικές απαιτήσεις, μπορείτε συνήθως να επιστρέψετε σε διάστημα 3–6 εβδομάδων, υπό την προϋπόθεση ότι μπορείτε να βαδίζετε με ασφάλεια και να μετακινείστε χωρίς σημαντικό πόνο. Σε αυτή τη φάση ενδέχεται να χρειάζεστε ακόμη βοήθημα βάδισης για μικρές αποστάσεις, γεγονός που δεν αποτελεί εμπόδιο σε καθιστική δραστηριότητα.
Αντίθετα, όταν η εργασία απαιτεί έντονη σωματική καταπόνηση, παρατεταμένη ορθοστασία, σκυψίματα ή άρση βαρών, το διάστημα αποχής παρατείνεται και μπορεί να φτάσει τις 6–8 εβδομάδες. Σε αυτές τις περιπτώσεις είναι απαραίτητη η πλήρης αποκατάσταση του εύρους κίνησης, η καλή μυϊκή ενδυνάμωση και η σταθερότητα του σκέλους, ώστε να μειωθεί ο κίνδυνος τραυματισμού ή υπερφόρτισης της νέας άρθρωσης.
Ο θεράπων ορθοπαιδικός, σε συνεργασία με τον φυσικοθεραπευτή, θα εκτιμήσει εξατομικευμένα την πρόοδό σας και θα σας δώσει κατευθυντήριες γραμμές για το πότε μπορείτε να επανέλθετε στην εργασία σας με ασφάλεια.
Μπορώ να κάνω ξανά αθλητικές δραστηριότητες και ποιες επιτρέπονται;
Η επιστροφή σε αθλητικές δραστηριότητες μετά από αρθροπλαστική γόνατος είναι εφικτή, ωστόσο προϋποθέτει ολοκληρωμένη αποκατάσταση, επαρκή μυϊκή ενδυνάμωση και πλήρη έλεγχο της νέας άρθρωσης. Οι δραστηριότητες χαμηλής έντασης, όπως περπάτημα, κολύμβηση, ποδήλατο, γιόγκα, θεωρούνται ασφαλείς και ενθαρρύνονται, καθώς συμβάλλουν στη βελτίωση της κινητικότητας και της φυσικής κατάστασης.
Αντίθετα, αθλήματα που επιβαρύνουν έντονα την άρθρωση, όπως το τρέξιμο σε μεγάλες αποστάσεις, τα άλματα ή τα ανταγωνιστικά αθλήματα με σωματική επαφή (π.χ. ποδόσφαιρο, μπάσκετ) καλό είναι να αποφεύγονται, καθώς ενδέχεται να προκαλέσουν μείζονα τραυματισμό. Σε ορισμένες περιπτώσεις μπορεί να επιτραπεί η σταδιακή επάνοδος σε πιο απαιτητικές δραστηριότητες, πάντα μετά από εξατομικευμένη εκτίμηση του Ορθοπαιδικού.
Θα μπορώ να γονατίζω ή να ανεβαίνω σκάλες κανονικά μετά την επέμβαση της αρθροπλαστικής γόνατος;
Το γονάτισμα και η άνετη ανάβαση κλίμακας μετά από αρθροπλαστική γόνατος αποτελούν εύλογες ανησυχίες, καθώς σχετίζονται άμεσα με την ποιότητα της καθημερινής λειτουργικότητας. Στις περισσότερες περιπτώσεις, οι ασθενείς μπορούν να ανεβαίνουν και να κατεβαίνουν σκάλες σχετικά σύντομα, συνήθως μέσα στις πρώτες ημέρες, χρησιμοποιώντας βοηθήματα βάδισης. Με την πρόοδο της μυϊκής ενδυνάμωσης και της αποκατάστασης του εύρους κίνησης, η λειτουργία αυτή γίνεται ολοένα και πιο φυσιολογική, αν και μπορεί να απαιτηθεί διάστημα μερικών εβδομάδων μέχρι να εκτελείται με πλήρη άνεση.
Το γονάτισμα αποτελεί πιο σύνθετο ζήτημα. Παρά το γεγονός ότι η πρόθεση είναι σχεδιασμένη να επιτρέπει μεγάλο εύρος κάμψης, πολλοί ασθενείς αναφέρουν δυσφορία ή αίσθημα πίεσης κατά την πλήρη κάμψη, ακόμη και αρκετούς μήνες μετά την επέμβαση. Αυτό δεν σημαίνει ότι η κίνηση είναι επικίνδυνη για την άρθρωση, αλλά συχνά σχετίζεται με την ευαισθησία των μαλακών μορίων στην πρόσθια επιφάνεια του γόνατος. Όμως, με την κατάλληλη φυσικοθεραπεία, μετά από μερικούς μήνες, οι ασθενείς που έχουν υποβληθεί στην επέμβαση μπορούν να γονατίζουν χωρίς περιορισμούς.
Πότε θα μπορώ να οδηγήσω ξανά;
Η επάνοδος στην οδήγηση μετά από την επέμβαση της αρθροπλαστικής γόνατος αποτελεί μια από τις συχνότερες απορίες. Ο χρόνος επιστροφής στην οδήγηση καθορίζεται από το αν η επέμβαση έγινε στο δεξί ή στο αριστερό γόνατο, από την ταχύτητα της αποκατάστασης και από την ικανότητα του ασθενούς να ανταποκρίνεται άμεσα σε απρόβλεπτες καταστάσεις κατά την οδήγηση.
Συνήθως, για το δεξί γόνατο απαιτείται διάστημα περίπου 4–6 εβδομάδων, καθώς είναι υπεύθυνο για τον χειρισμό των πεντάλ. Για το αριστερό γόνατο, εφόσον ο ασθενής οδηγεί όχημα με αυτόματο κιβώτιο ταχυτήτων, η οδήγηση μπορεί να ξεκινήσει νωρίτερα, ενίοτε και μετά την 3η εβδομάδα. Προϋπόθεση για την ασφαλή οδήγηση αποτελεί η επίτευξη ανώδυνης βάδισης, ο επαρκής νευρομυϊκός έλεγχος του σκέλους και η ικανότητα εκτέλεσης ταχείας κίνησης φρεναρίσματος.
 Hip Osteoarthritis
Hip Osteoarthritis

 +30 210 7292002
+30 210 7292002
 alilikakis@yahoo.com
alilikakis@yahoo.com