Carpal tunnel syndrome

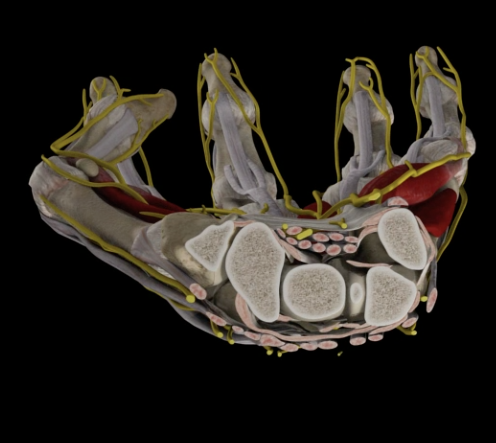
The “carpal tunnel” is a narrow tube on the palmar surface of the wrist. The “floor” of the tube is formed by the bones of the wrist while its “roof” is formed by a strong bundle of connective tissue called the “transverse ligament of the wrist”. Inside the tube passes the median nerve, which provides sensation to the palmar side of the thumb, index finger, middle finger and half (towards the thumb) fourth finger. It also controls the mobility of the thumb muscles (thenaros). The (eight) tendons that bend the four fingers of the hand also pass through the tube.
Carpal tunnel syndrome (CCS) occurs when the tissues surrounding the flexors of the wrist swell, narrow the limited space of the carpal tunnel and, over time, the nerve is pressed. In most cases of MS there is no specific cause, but several causes can contribute to its development:
1. Heredity: The carpal tunnel may be narrower in some people
2. intense hand activity: MS occurs most often in people with manual occupations or computer operators
3. Age: The disease occurs more often in older people.

4. Recent fractures of the wrist
5. Diseases, such as diabetes, rheumatoid arthritis and thyroid gland disorders, contribute to the appearance of the syndrome.
The most common symptoms of MS are:
1. Numbness (numbness), paresthesia (tingling) and pain in the wrist and hand, which worsen during the night or early in the morning and may radiate to the entire upper limb.
2. Feeling of electric current in the thumb, index and middle finger.
3. Decrease in the grasping power (dragmu) of the hand and, in advanced stages of the disease, atrophy of the muscles of the Thenaros.
4. Decrease in mobility (stiffness) of the wrist and hand and a feeling of clumsiness/weakness for fine movements resulting in falling objects.

Symptoms usually begin gradually and, in most people, are more severe on the thumb side. Symptoms can occur at any time, but at night they are more intense and can wake up the patient. During the day they usually appear in the prolonged raising of the hand, while driving or typing on a computer. Sudden hand movements (shakes) often help reduce discomfort. Symptoms initially present with flare-ups and remissions, but over time they can become permanent.
The clinical examination of the hand to diagnose MS consists of a series of tests such as:
1. Checking for weakness of the muscles of the thenaros.
2. causing symptoms by bending the wrist for a few minutes (Phalen Test).
3. repeated impacts of the median nerve at the height of the wrist cause numbness or a feeling of electricity in the fingers (Tinel test).
4. finger sensitivity test.
The electrophysiological examination of the upper limb (electromyogram, EMG, motor conduction speeds, CTA and aesthetic treatment speeds, ATA) is the paraclinical examination of choice, with which the CRS is documented. It is performed by specialized doctors, usually neurologists or physiatrists, checks the functionality of the nerves of the upper limb (aesthetic and motor) and the consequent effect on the muscles of the area, and is able to prove the pressure of a nerve (but not in the very early stages) and its exact position (e.g. wrist, elbow, neck). In special cases, a radiological examination of the fruit may also be required.
For most patients, MS will gradually worsen. However, its development may be modified or interrupted in the early stages. For example, if the symptoms are related to an activity or profession, the situation can be improved by refraining from the activity that is responsible. Treatment of MS can be conservative or surgical. If diagnosed early, the syndrome can be relieved without surgery. In cases where the diagnosis is uncertain or symptoms are mild to moderate, the doctor will initially try conservative means, such as:
1. Nocturnal carpal splint that holds the wrist in a neutral position and prevents nerve irritation. It can also be worn during activities that worsen symptoms.
2. Medications: Non-steroidal anti-inflammatories can help relieve pain by acting de-swelling on the focus of the problem.
3. Modification of activities: If the demands of the job cause the symptoms, changing or modifying them, it can alleviate.
4. Topical injection of corticosteroids: Injecting cortisone into the wrist offers temporary relief for another period of time.
5. Physiotherapy (ultrasound, diathermy, TENS, etc.), may have a beneficial effect on relief by combating local irritation.
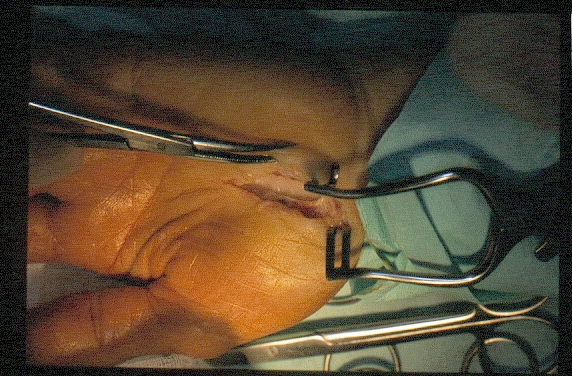
In case of failure of conservative treatment, surgical treatment will bring the definitive solution to the problem. In very severe cases, with constant numbness and weakening of the muscles of the thenaros, surgery is recommended immediately to prevent irreversible damage. Carpal tunnel syndrome surgery is performed under local anesthesia and lasts five to ten minutes. During the operation, a small incision is made in the palm, about two centimeters long. The transverse ligament of the wrist is located and intersected by automatically increasing the cross-sectional range of the carpal tunnel and relieving the nerve. The patient is immediately discharged from the hospital with medication (antibiotics, painkillers) and instructions to keep the limb in an upright position and move the fingers to avoid swelling and stiffness. Driving and self-service are allowed immediately after the operation. The doctor will decide on the return to work and any restrictions. Most patients see immediate improvement, but complete cure is gradual and, on average, takes about a month after surgery. In neglected MS, with severe loss of sensation and/or muscle atrophy, recovery is slower and may not be complete.
 Hip Osteoarthritis
Hip Osteoarthritis

 +30 210 7292002
+30 210 7292002
 alilikakis@yahoo.com
alilikakis@yahoo.com