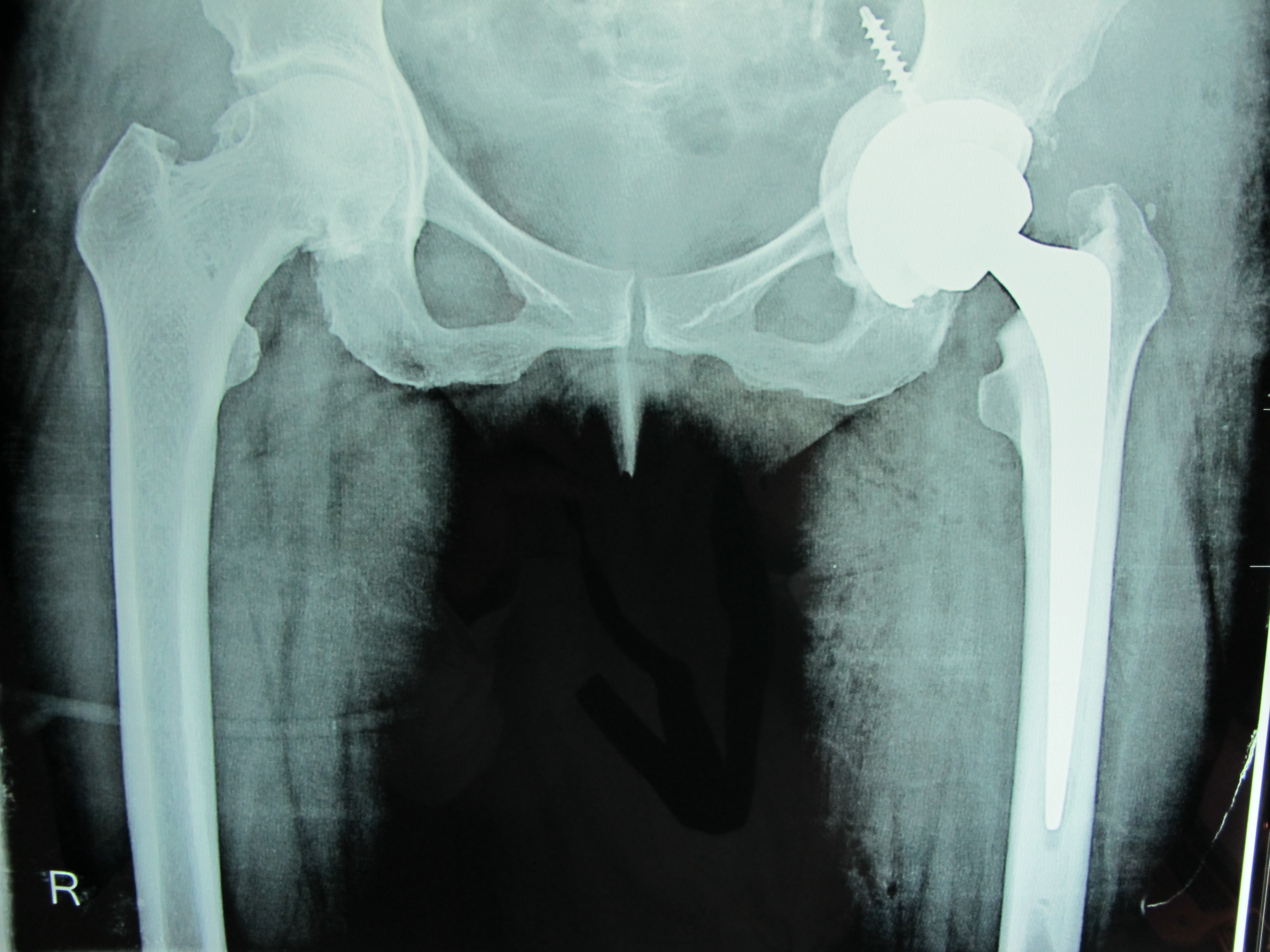
Total Hip Arthroplasty
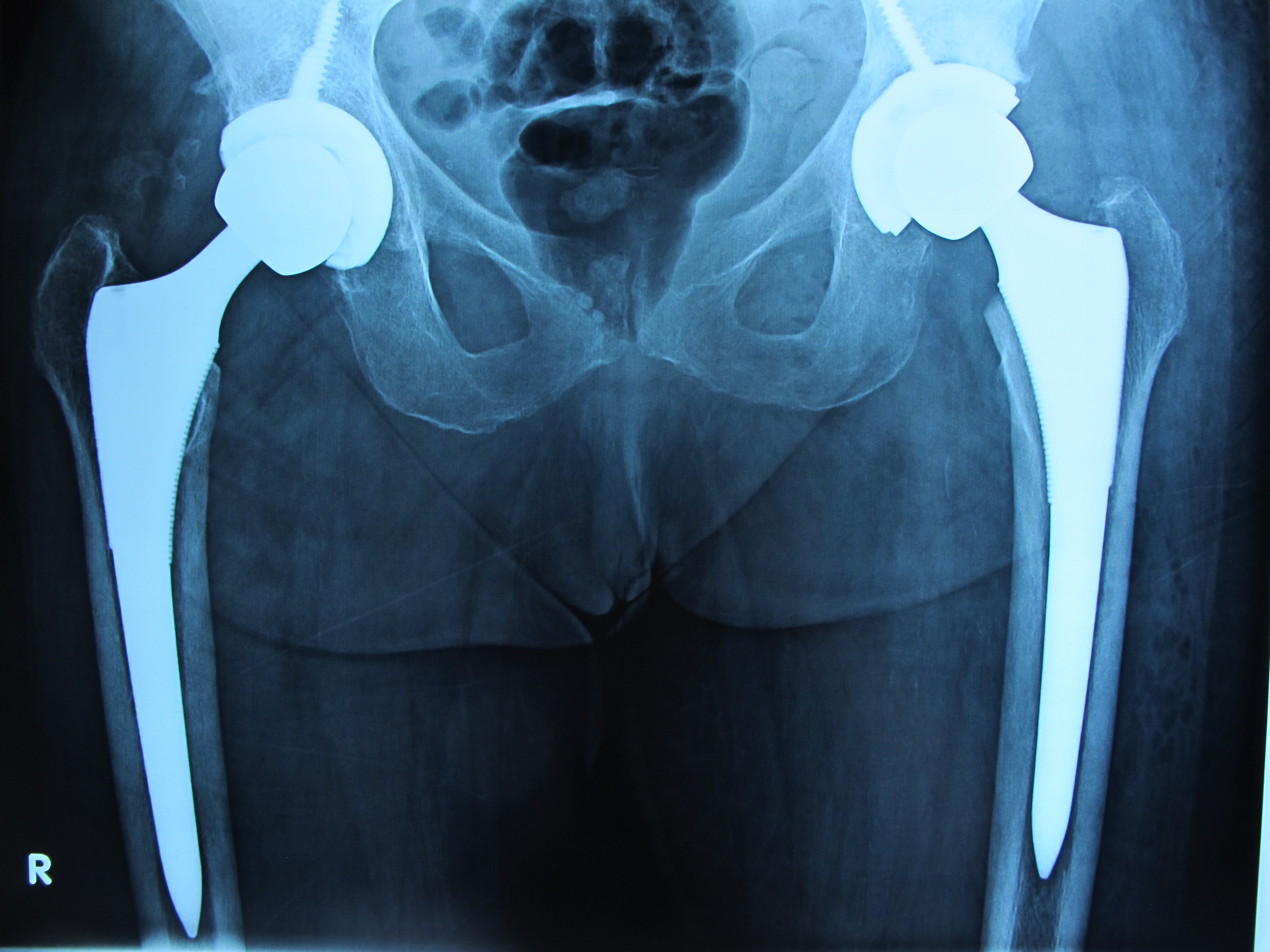
Total hip arthroplasty is the surgical procedure to completely repair a damaged hip joint. That is why it is alternatively called total hip replacement. With the development of surgical techniques and implants, its effectiveness in hip reconstruction is approaching perfection and for this reason it has been characterized as the surgical intervention of the20th century. When conservative treatment fails, total hip replacement is the only effective and documented solution to relieve the patient.
Why replace the hip?
There are three main reasons that can lead to hip replacement:
- Pain: it is caused due to the destruction of the joint and is the predominant symptom when we decide to replace the hip. It can be non-stop, dominate every aspect of life, and make physical activity nearly impossible.
- Deformity: Sometimes the hip can be deformed and in a contraction so that the body leans forward. Due to the deformity, there is often a shortening of the strand. The presence of a stiff hip puts a strain on the lumbar. Replacing the affected hips therefore protects and relieves the spine.

Lameness: Both the pain and shortening of the leg, as well as the muscle atrophy from the prolonged attack of the joint cause lameness and the patient comes for surgery because he is visibly limp.
When do I need a total hip arthroplasty?
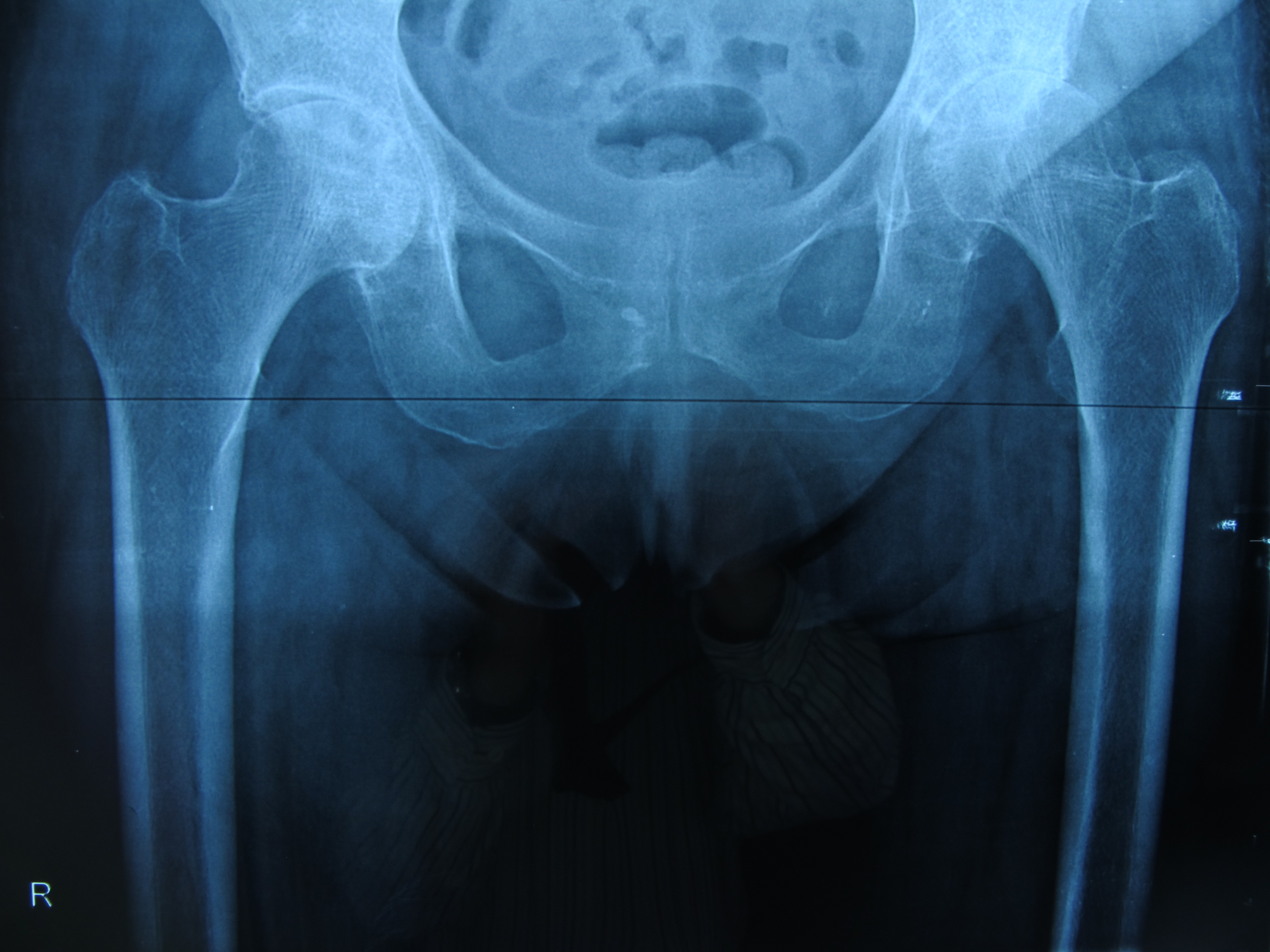
You may need a total hip replacement if your hip joint is damaged by various types of arthritis, the main ones being:
- osteoarthritis, which is the most common
- rheumatoid arthritis or other rheumatic diseases
- post-traumatic arthritis
It is important to note that not all patients with hip arthritis undergo total arthroplasty. It is only recommended when the pain and disability caused have significant effects on your daily activities. Initially, your doctor will attempt to relieve you with other treatments, such as painkillers or anti-inflammatories, a bacterium or physical therapy. The final decision is made by the patient himself, who judges whether he needs to undergo surgery by the extent to which arthritis affects his life.
What can I expect from a total hip arthroplasty?
The main benefit of surgery is the elimination of pain and deformity. You will usually notice pain remission immediately after surgery. You will also get:
- much greater mobility.
- greater range of motion in your hip.
- better quality of life.
However, an artificial joint is never as good as your normal hip when it was healthy. There are some limitations.
Preparation for hip arthroplasty
Total hip arthroplasty is a major surgical procedure and any patient can help in its rehabilitation. This can be achieved by being better prepared. The best way to make the operation as easy as possible is to be in good general health before surgery.
Steps to prepare for hip arthroplasty
- SMOKING RESTRICTION : Smokers are more vulnerable to respiratory complications during anesthesia. They are also prone to respiratory infections after surgery. This can prolong the period of bedtime and delay the patient’s progress.
- WEIGHT LOSS: An overweight patient is more difficult to operate on than a thin one because the hip is covered by a greater mass of soft tissues., which leads to more bleeding. Overweight patients are also more vulnerable to breathing problems during anesthesia and postoperative hip infections. Patients should lose as much weight as possible. Less weight will also subject future arthroplasty to smaller loads.
- MEDICATION ADJUSTMENT: Medications for the heart, arterial hypertension, diabetes mellitus, or any condition the patient has should be taken systematically so that the patient is in the best possible condition. It is useful for the patient to visit his respective treating doctors before the operation.
- EXERCISE : Patients should do any physical exercise they can, as this will make it easier for them to return to normal activity after surgery. The hospital physical therapist may recommend exercises to strengthen specific muscle groups in the body.
- SPACE PREPARATION: Small changes in the home may be necessary to prepare for the return after surgery. For example, the seats should not be too low, while for the basins a special lifting seat is needed. In addition, the beds should be neither too soft nor too low. Such information will be given to you by your surgeon.
What happens before hip arthroplasty?
Upon admission to the hospital
Total arthroplasty surgery can be performed under general or regional anesthesia. As with other major surgeries, the patient should undergo a preoperative check-up. A complete medical history is usually taken and various laboratory tests are performed. Examples of such tests are listed below:
- BLOOD TESTS : To check hematocrit, kidney function, electrolytes, etc. Blood will also be taken for cross-referencing, so that blood is available in the rare event that a transfusion is required.
- URINE TESTS: They are necessary to check for a possible urinary tract infection before surgery. If this is the case, it is very likely that total arthroplasty will be postponed, as it can be infected by an existing urinary tract infection.
- RADIOLOGICAL EXAMINATION: Chest X-ray to check the heart and respiratory.
- RADIOLOGICAL EXAMINATION OF THE HIP: Necessary for preoperative planning by the surgeon.
- ELECTROCARDIOGRAM : Checks the rhythm and other parameters of the heart.
Admission to the hospital usually takes place on the morning of the day of surgery. Preventive medication (anticoagulants) will be given to reduce the risk of venous thrombosis. Antibiotics are also administered to reduce the very small but real risk of perioperative infection after surgery.
What happens on the day of hip arthroplasty?
The preoperative check-up is usually done a few days before admission for surgery, while the admission is done on the eve or early of the same morning of the operation. Rarely, if there are any known, serious health problems (cardiological, respiratory, etc.), it may be advisable to admit you 1-2 days earlier than usual to regulate them.
Anesthesia
In the operating room, you will be given anesthesia by the anesthesiologist. It can be general anesthesia (in this case you will sleep) or a local – strain anesthesia, such as epidural or spinal anesthesia. In this case you have no sensation and pain from the waist down. Most patients today are operated on under spinal or epidural anesthesia. At the same time, they are also subjected to a slight “intoxication” during the operation so that they do not hear and understand what is happening. When you enter the operating room, you will be placed:
- on the side on the healthy hip in order to perform the surgery with the posterior access (MIS posterior)
- supine position in the case of Direct Anterior Approach (DAA).
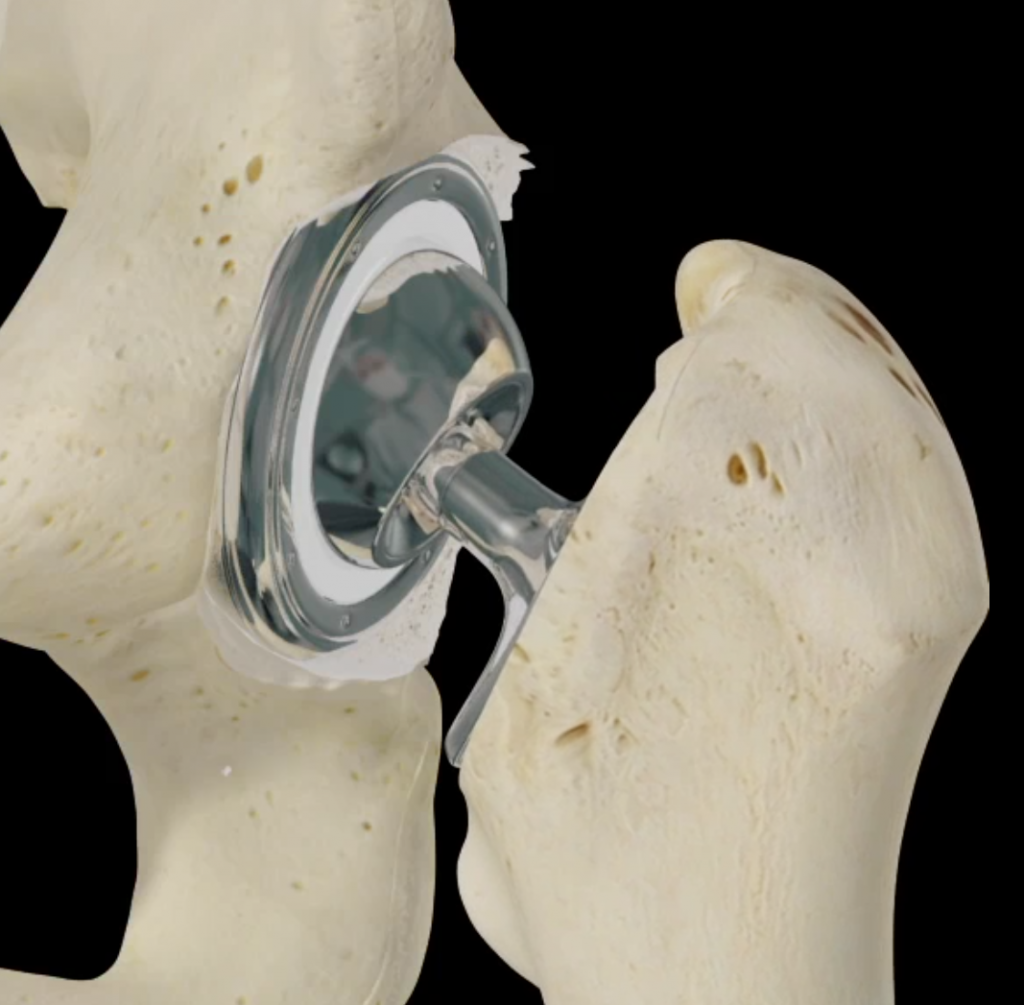
Hip arthroplasty
During surgery, the arthritic part of the hip joint is removed and artificial prostheses are inserted. The incision can be from 10 to 15 points approximately. It depends on the dimensions, general and local, of the patient, and on the technique to be applied. Newer techniques, which include the so-called Minimally Invasive Technique (MIS), generally require smaller incisions and more non-traumatic surgical approaches. As a result:
- Blood loss is limited
- Muscle damage in the area is limited
- the chances of developing postoperative complications are reduced, and
- The return to daily activities is accelerated.

However, they are done with specific criteria and in selected patients. Making a general reference, the more thickness or fat there is around the joint the larger the incision will be needed. This is due to the fact that the joint is more “hidden” and a disclosure should be made that allows the implants to be placed correctly and accurately.
The procedure
The surgeon cuts and opens the skin and the tissues, muscles and ligaments below it in order to expose the hip joint. The hip is then dislocated and the femoral head is removed with a special saw. By removing the femoral head, the acetabulum is revealed. The residual cartilage and arthritic bone of the acetabulum are removed with special surgical instruments called relicts, which rotate quickly and “eat” the arthritic bone. It is important to remove all the affected bone leaving behind healthy, bleeding bone. Healthy bone will accept the acetabular implant much better than arthritic bone.
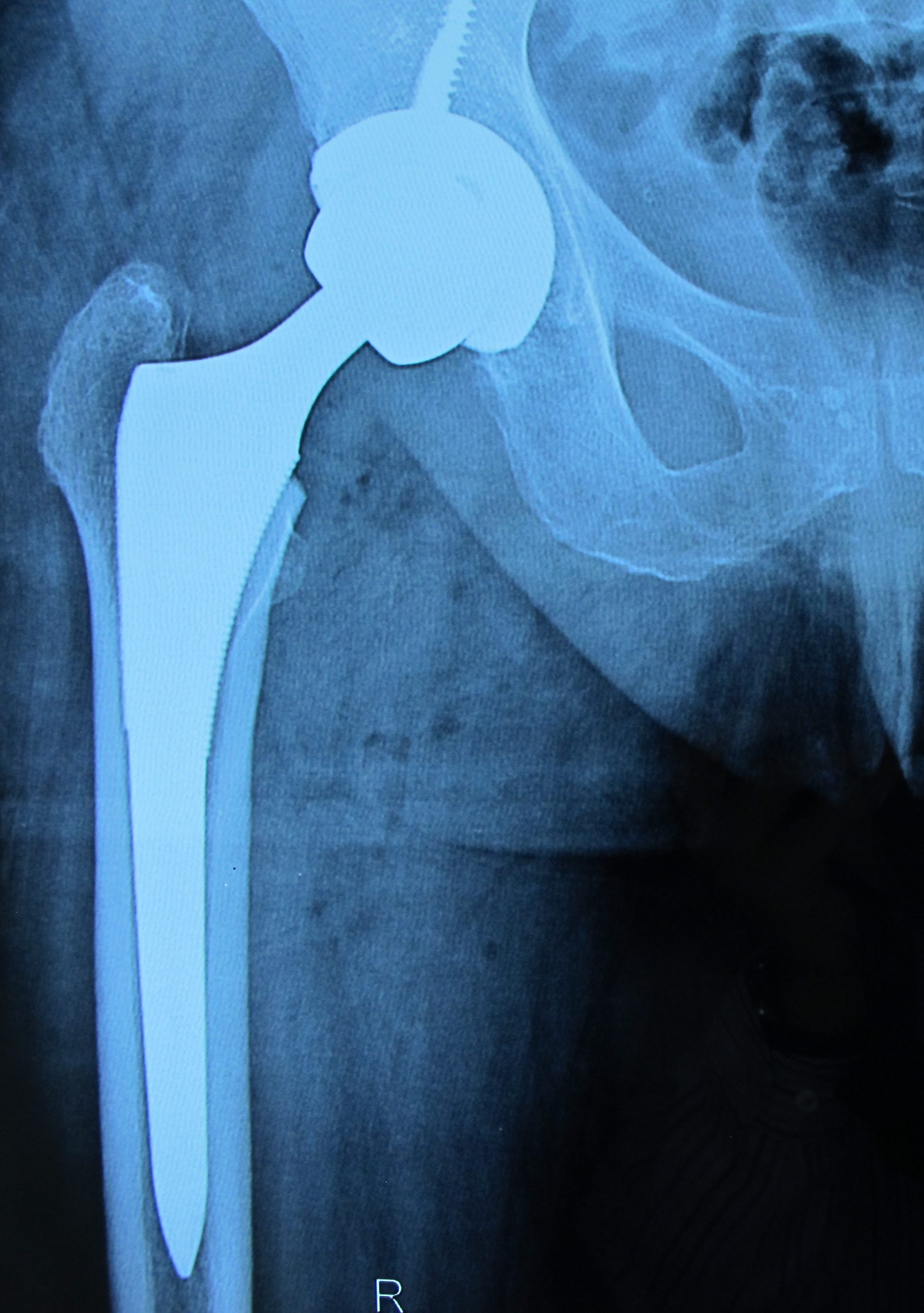
The first implant to be placed is the acetaminophen implant. Once it has been placed in the acetabulum, the femur is then prepared again with special tools, called “rasps” and the femoral implant (femoral spine) is placed. Then the head (“head”) is placed in the femoral stem, which fits into the acetabulum. Once the three implants have been placed firmly, then the hip is rearranged in place, i.e. the head enters the acetabulum. At the same time, the various layers of subcutaneous and skin are sutured or repositioned in their original position.
How long does it take to heal?
The new joint is held in place by the surrounding muscles and soft tissues which will strengthen during the time the wound heals, with the necessary condition of course being the correct placement of the implants. It usually takes a period of around 40 days for the soft tissues that were damaged during surgery to heal. During this time, further attention will be needed from the patient.
No matter how hard the surgeon tries to perform hemostasis in the operating room area, it is not possible to stop all the bleeding during the operation. So nature will do the rest of the work in the first 24 hours after surgery by activating the body’s clotting factors.
How is implant fixation done?
There are two ways to stabilize implants in the bone:
- with the use of bone cement, which offers immediate stabilization and is usually used at older ages or on osteoporotic hips
- by embedding them and biologically integrating them over time into younger individuals.
Fixation in the acetabulum was traditionally done with bone cement, a technique that is still used in some cases successfully. The usual practice, however, is cement-free fastening. The acetabular implant (acetabular prosthesis) has a special configuration – treatment on its surface. They are tracheal and often with a special coating (such as hydroxyapatite), with which the interconnection of the bone with the prosthesis is achieved. On the other hand, the femoral swab is stabilized in the lumen of the femur either with the use of cement, which is still used for the femoral prosthesis, or, more often, without the use of cement. In this case, too, the interconnection of the femoral swab with the bone is achieved by properly treating its surface, which is porous, as well as by coating it with special materials.
What material are implants made of?
The acetaminophen implant usually consists of titanium-based metal alloys , when placed without cement. A polyethylene (plastic) insert is placed inside which will be articulated with the head. When the fastening is done with cement, it consists entirely of UHMWPE polyethylene, very high molecular weight. Newer techniques and discoveries have led to the creation of inserts other than polyethylene, such as ceramic or metal, which achieve less friction with a longer lifespan. They are usually used at younger ages.
The head can be metal if it is articulated with plastic or metal, or it can be ceramic when articulated with plastic or ceramic. The femoral swab respectively is made of titanium-based metal alloys if fastened without cement and chromocobalt-based if fastened with cement.
What is surface arthroplasty?
Sometimes it is preferred to replace the head completely or replace only the surface of the femoral head, in order to achieve the removal of the smaller amount of bone and the use of a larger articulated surface. This operation is called surface arthroplasty. Hinged surfaces are metal to metal. The operation is performed on younger people as it achieves:
- Greater range of motion
- better possibility of sports activities
- greater ease in the next operation, when and when it is required.
Nevertheless, metal-to-metal surface arthroplasty is not indicated, among other things, in cases of:
- osteoporotic bone, because a fracture of the femoral neck can occur.
- in young women of childbearing age.
- people with a small skeleton.
- patients with a metal allergy.
What happens after hip arthroplasty?
When you leave the operating room you will usually have a venous catheter in your hand to administer fluids and medication. You will be taken to the recovery room where you will stay until you fully recover and are in a stable hemodynamic state so that you can be transferred to your room. You will be given painkillers to relieve postoperative pain, antibiotics and other medications to prevent vomiting, constipation and more.
A few hours after the surgery you will be able to turn to the side, sit sitting in bed, stand up and walk with a walker or a pair of bacteria with the instructions and care of a physiotherapist. There is a specific way to perform all these activities, which will be explained to you in detail by your physiotherapist and doctor. How quickly you will return to your normal activity depends on many factors, including:
- Age and weight
- The condition you were in before the surgery,
- Your overall health
- The condition of the rest of your joints.
Physiotherapy and learning after hip arthroplasty.
Physiotherapists will help you move comfortably and teach you the exercises to strengthen the muscular system. They will explain to you which movements are allowed and which are prohibited in the first time after a total hip arthroplasty. It is very important that you follow these rules. For example, you should avoid bending your hips too much, such as sitting low and crossing your legs. These restrictions usually apply, along with others, for the first postoperative month. They will explain to you what is the right way to:
- get out of bed
- Sit
- walk
- to go up and down the scale
- go to the toilet.

When can I leave the hospital after hip arthroplasty?
Most patients are able to climb the stairs and walk with assistance within 24-36 hours. Therefore, then they can leave the hospital. The stitches are removed after 2-3 weeks. The surgeon will want to see you again, usually within 40-50 days of surgery, with a new x-ray.
What happens in the first few weeks after hip arthroplasty?
You’ll find that you can flex your hip toward your belly as much as you’d like, but it’s important not to attempt it to see its limits at first. You need to be careful in the first 8-12 weeks after surgery.
You may be able to drive a car after the first month and return to work at the same time if your job does not require manual labor or a lot of commuting. Getting in and out of the car can be difficult at first. You may need to sit on your side, in the seat first, and then bring your feet in. These will have been explained to you by your physiotherapist at the hospital. You must do your exercises regularly.
Walking, swimming (but not breaststroke) and cycling are exercises that you can do after 4 – 8 weeks. However, you should avoid running on hard surfaces, doing sports that involve intense physical contact, are at a high – competitive level, as they subject your hip to great forces.
What are the long-term effects of total hip arthroplasty?
There are many different types of arthroplasty today. Some may be better than others, but there are many factors that affect the outcome and survival of an artificial one. You should expect your arthroplasty to last at least 15-20 years. As a rule, in younger patients under 50 years of age, arthroplasty survives fewer years because the patient’s demands are much greater and the stresses on the artificial joint are greater.
Can there be complications from hip arthroplasty?
Total arthroplasty is a major surgical procedure and can rarely have complications. The risk varies depending on the general state of health of the patient. Therefore, you need to discuss the potential risks and complications with your surgeon. The patient must be fully informed before proceeding with the operation (“informed written consent”).

Complications can occur during or after surgery. They can also be divided into those that occur as a result of any major surgery (general complications) and those that are specific to total hip arthroplasty (specific complications).
General complications:
- Hematoma, in the wound or internally: sometimes there can be a collection of blood in the surgical field. It rarely needs to be drained, which requires a small opening of the wound.
- Wound splitting: this means that the wound “opens” and it will have to be re-closed – sutured.
- Complications from the urinary tract: it is common for patients to have difficulty urinating after surgery. This is the result of the difficulty that some patients have to urinate when lying down, which probably existed before the surgery. It is more common in men with prostatic hypertrophy. To treat these problems, a catheter is sometimes placed to empty the bladder for a few days after the operation.
- Gastrointestinal complications: The intestine has underactive activity for a few days. This is usually treated with appropriate medication with laxatives. It should be noted that both reduced patient mobility and analgesic drugs can cause constipation which is successfully treated with laxatives.
- Respiratory complications: usually occur as a result of anesthesia and bedsores. Patients with previous heart or respiratory problems are more prone to these types of complications.
- Circulatory complications: After total hip arthroplasty, a possible complication is deep vein thrombosis (DVT), which affects the veins of the lower limbs. Fortunately, this complication is not common. In addition, it can be prevented by using appropriate medication. In the event that it happens, it is treated again with appropriate medication. There is a more serious complication in which clots can detach from veins in the lower extremities (in case of DVT) and migrate to the lungs (pulmonary embolism, PE). PE is a very serious complication but it is extremely rare.
Specific complications:
- Dislocation: The artificial joint can dislocate, usually after some incorrect or sudden movement. This happens in less than 1 in 100 cases, and the hip is placed in place under anesthesia. Usually this alone is enough to make the hip stable. However, in some cases, patients may need to do additional exercises to strengthen the muscles around their hip. Very rarely, a new operation may be necessary, usually in cases of repeated dislocations.
- Fracture: It occurs at a rate of less than 0.5% for the initial arthroplasty and about 3% for the revision of the arthroplasty. This usually happens during the operation as a result of the high forces to which the bone is subjected in the operating room. If it is noticed during the operation, the surgeon usually treats the issue immediately, either using stiffener wires or screws and plates. Otherwise, prolonged lying down is recommended so that the fracture heals naturally.
- Nerve injury during surgery (maximum 2%): As nerves pass very close to the hip joint, it is not surprising that they can be injured. Most of the time, resuscitation occurs automatically during a period, usually around a year.
- Persistent pain around the major trochanter: Known as “trochanteritis” it can be localized pain on the outer surface of the hip. It has no functional significance but can be annoying for the patient.
- Implant movement: In this the artificial hip changes position inside the joint. It is very rare, but occasionally implants can become embedded in the bone. A femoral stem, for example, can be immersed inside the femur, while a acetabular implant can be immersed inside the acetabulum. It is usually the result of weakness of the patient’s supporting bone.
- Leg length difference: One of the relatively common complications of total hip arthroplasty is the creation of a leg discrepancy. It is more common for the operated leg to become longer and there is sometimes a need for a shoe lift on the other leg to compensate for this difference. However, it must be made clear that it is a basic concern of the surgeon to count the legs during and at the end of the operation in order to create a complete balance which is not always entirely possible.
- Infection: In order to prevent infections, special operating rooms are used in which the air is renewed and the microbial load is reduced. Patients are given antibiotics during and after the operation, for the same reason. Nevertheless, the risk of a deep infection exists, but in less than 1 in 200 cases. And this is a serious complication because the artificial joint may need to be removed until the infection is eradicated. A new joint will be inserted 6-9 weeks later.
- Damage to vessels : As with nerves, so with large vessels that pass around the hip joint and can be injured during an operation. This complication, however, is extremely rare.
Why should I choose Dr. Anastasios Lilikakis for total hip arthroplasty?
Total hip arthroplasty is a complex yet effective solution for treating damaged joints. The replacement of the joint should be done exclusively by an experienced and qualified Orthopedic Surgeon, as it requires precision and attention to movements.
Dr. Anastasios Lilikakis has many years of experience and expertise in hip surgery using all modern surgical techniques. He is the Chairman of the Department of Hip & Knee Reconstructive Surgery, which is the scientific and educational arm of the Hellenic Orthopaedic Society. If you have problems with your hip, contact your Orthopedic Surgeon, Dr. Anastasios Lilikakis for early diagnosis and the right choice of treatment method for your case. Contact us immediately to book your appointment.
Θα μπορώ να περπατήσω αμέσως μετά την επέμβαση της αρθροπλαστικής ισχίου;
Στις περισσότερες περιπτώσεις οι ασθενείς ενθαρρύνονται να σηκωθούν και να περπατήσουν πολύ σύντομα μετά την αρθροπλαστική ισχίου, συνήθως την ίδια ημέρα. Αυτό γίνεται πάντα υπό την καθοδήγηση του ιατρού και του φυσικοθεραπευτή, με τη βοήθεια ειδικών βακτηριών (πατερίτσες) ή περιπατητήρα «πι». Η πρώιμη κινητοποίηση είναι ιδιαίτερα σημαντική, καθώς μειώνει τον κίνδυνο επιπλοκών, όπως η θρόμβωση, και συμβάλλει στη γρηγορότερη αποκατάσταση της λειτουργικότητας του ισχίου. Η ένταση και η διάρκεια του βαδίσματος αυξάνονται σταδιακά, ανάλογα με την πρόοδο του ασθενούς και τις οδηγίες της ιατρικής ομάδας.
Είναι ασφαλές να ανέβω και να κατέβω σκάλες μετά την επέμβαση;
Μετά την αρθροπλαστική ισχίου, η χρήση σκάλας είναι εφικτή σχετικά σύντομα, αλλά απαιτείται ιδιαίτερη προσοχή και πάντοτε καθοδήγηση από την ιατρική ομάδα. Στις περισσότερες περιπτώσεις, οι ασθενείς εκπαιδεύονται ήδη από τη νοσηλεία τους από τον φυσικοθεραπευτή, ο οποίος δείχνει τον σωστό τρόπο ανόδου και καθόδου της κλίμακας. Με την πάροδο των ημερών και την ενδυνάμωση των μυών, η διαδικασία γίνεται πιο ασφαλής και άνετη. Συνήθως, μέσα στις πρώτες ημέρες, οι περισσότεροι ασθενείς μπορούν να χρησιμοποιούν σκάλες με σταθερότητα και όλο και λιγότερη υποστήριξη.
Πότε μπορώ να επιστρέψω στη δουλειά μου μετά από την επέμβαση της αρθροπλαστικής ισχίου;
Η επιστροφή στην εργασία μετά από αρθροπλαστική ισχίου εξαρτάται από πολλούς παράγοντες, όπως το είδος της εργασίας, η ηλικία και η γενική φυσική κατάσταση του ασθενούς. Για άτομα με καθιστική εργασία, η επιστροφή στην εργασία μπορεί συνήθως να πραγματοποιηθεί σε διάστημα περίπου 4 έως 6 εβδομάδων.
Αντίθετα, σε επαγγέλματα που προϋποθέτουν έντονη σωματική δραστηριότητα, ο απαιτούμενος χρόνος ανάρρωσης είναι μεγαλύτερος και μπορεί να φτάσει τους 2 έως 3 μήνες, προκειμένου να διασφαλιστεί η ομαλή αποκατάσταση και να περιοριστεί ο κίνδυνος τραυματισμού. Είναι σημαντικό ο ασθενής να ακολουθεί πιστά το πρόγραμμα φυσικοθεραπείας και τις οδηγίες του θεράποντος Ορθοπαιδικού, καθώς η ασφαλής επιστροφή στην εργασία αποτελεί εξατομικευμένη απόφαση και δεν πρέπει να γίνεται βιαστικά.
Πότε θα μπορέσω να επιστρέψω στις αθλητικές μου δραστηριότητες μετά την επέμβαση;
Η επιστροφή στις αθλητικές δραστηριότητες μετά από αρθροπλαστική ισχίου γίνεται σταδιακά και πάντοτε με γνώμονα την ασφάλεια του ασθενούς. Οι ήπιες μορφές άσκησης, όπως η κολύμβηση, επιτρέπονται συνήθως μέσα στους πρώτους 1 με 2 μήνες, καθώς συμβάλλουν στην ενδυνάμωση των μυών, στη βελτίωση της κινητικότητας και στην ψυχολογική ανάκαμψη. Αθλήματα με μεγαλύτερες απαιτήσεις, όπως το ποδήλατο ή το γκολφ, μπορούν να ενταχθούν σταδιακά μετά το πέρας δύο μηνών, εφόσον η ανάρρωση εξελίσσεται ομαλά και χωρίς επιπλοκές. Οι δραστηριότητες υψηλής καταπόνησης (π.χ. τρέξιμο ή ομαδικά αθλήματα με απότομες αλλαγές κατεύθυνσης ή σωματική επαφή ) συνήθως αποθαρρύνονται για τους πρώτους έξι μήνες, ώστε να προστατευθεί η πρόθεση και να αποφευχθούν τυχόν εξαρθρήματα. Η τελική απόφαση για την επιστροφή στην άθληση λαμβάνεται εξατομικευμένα, μετά από αξιολόγηση του θεράποντος ιατρού και σε συνεννόηση με τον φυσικοθεραπευτή.
Θα έχω πρόβλημα με τους ελέγχους ασφαλείας στα αεροδρόμια λόγω της πρόθεσης;
Η ύπαρξη μεταλλικής πρόθεσης στο ισχίο μπορεί πράγματι να ενεργοποιήσει τους ανιχνευτές μετάλλων κατά τον έλεγχο ασφαλείας στα αεροδρόμια. Αυτό δεν αποτελεί ιατρικό πρόβλημα, αλλά μια συνηθισμένη πρακτική δυσκολία που αντιμετωπίζουν πολλοί ασθενείς μετά από αρθροπλαστική. Σε αυτές τις περιπτώσεις, συνήθως πραγματοποιείται ένας σύντομος επιπλέον έλεγχος από το προσωπικό ασφαλείας. Δεν απαιτείται κάποιο ειδικό έγγραφο, ωστόσο είναι χρήσιμο να ενημερώνετε εκ των προτέρων τους υπευθύνους για την ύπαρξη πρόθεσης. Σε κάποιες περιπτώσεις μπορεί να χορηγηθεί σχετική βεβαίωση, αν και αυτό δεν είναι τυπικά υποχρεωτικό. Σε κάθε περίπτωση, η διαδικασία ελέγχου ολοκληρώνεται χωρίς προβλήματα και δεν επηρεάζει την καθημερινότητά σας ή την ικανότητα να ταξιδεύετε. Να θυμάστε ότι η αρθροπλαστική είναι μία πολύ συνηθισμένη επέμβαση και οι υπάλληλοι στα αεροδρόμια είναι εξοικειωμένοι.
Τι πρέπει να προσέχω στο σπίτι τις πρώτες εβδομάδες μετά την αρθροπλαστική ισχίου;
Τις πρώτες εβδομάδες στο σπίτι μετά από αρθροπλαστική ισχίου, η προσοχή επικεντρώνεται στην ασφάλειά σας και στη σωστή αποκατάσταση. Είναι σημαντικό να αποφύγετε κινήσεις που θέτουν σε κίνδυνο την πρόθεση, όπως το να σκύβετε πολύ χαμηλά, να σταυρώνετε τα πόδια ή να κάθεστε σε πολύ χαμηλές καρέκλες. Ο χώρος του σπιτιού καλό είναι να προσαρμοστεί κατάλληλα (πχ. απομάκρυνση χαλιών που γλιστρούν, τοποθέτηση βοηθητικών χειρολαβών στο μπάνιο ή στις σκάλες κ.ά.) Η χρήση βακτηριών θα σας προσφέρει σταθερότητα στο περπάτημα. Παράλληλα, πρέπει να ακολουθείτε πιστά τις οδηγίες του θεράποντος ιατρού και του φυσικοθεραπευτή σχετικά με τις ασκήσεις και τη φαρμακευτική αγωγή. Με αυτόν τον τρόπο μειώνεται ο κίνδυνος επιπλοκών και υποστηρίζεται η ομαλή ανάρρωση.
Η πρόθεση έχει διάρκεια ζωής; Χρειάζεται αλλαγή μετά από χρόνια;
Οι σύγχρονες προθέσεις ισχίου χαρακτηρίζονται από υψηλή αντοχή, η οποία στις περισσότερες περιπτώσεις υπερβαίνει τα 20-25 έτη. Η φθορά της πρόθεσης εξαρτάται από πολλούς παράγοντες, όπως η ηλικία και το σωματικό βάρος του ασθενούς, το επίπεδο καθημερινής δραστηριότητας, καθώς και η παρουσία συνοδών παθήσεων. Σε ορισμένα περιστατικά, ενδέχεται με την πάροδο του χρόνου να εμφανιστεί χαλάρωση ή φθορά της πρόθεσης, γεγονός που μπορεί να απαιτήσει αναθεώρηση της αρθροπλαστικής. Όμως, η πρόοδος της τεχνολογίας, η χρήση βιοσυμβατών υλικών και οι σύγχρονες ελάχιστα επεμβατικές τεχνικές έχουν μειώσει σημαντικά την ανάγκη για επανεπεμβάσεις. Η τακτική παρακολούθηση από τον θεράποντα ορθοπαιδικό κρίνεται ουσιώδης για την έγκαιρη ανίχνευση πιθανών επιπλοκών και τη διασφάλιση της απρόσκοπτης λειτουργίας της πρόθεσης στο πέρασμα του χρόνου.
 Hip Osteoarthritis
Hip Osteoarthritis

 +30 210 7292002
+30 210 7292002
 alilikakis@yahoo.com
alilikakis@yahoo.com