History and Evolution of Total Knee Arthroplasty
The evolution of total knee arthroplasty
Total knee arthroplasty is not a new operation. In the 1930s, the operation of semi-arthroplasty was performed, i.e. the replacement of half of the joint. This was followed by a period of replacement of the joint with materials known as restrictive type arthroplasties. These arthroplasties were like the “hinge” of the door, that is, they only allowed the bending and extension of the knee.
However, it is now known that the normal knee does not only flex and extend, that is, it does not only bend and stretch, but also makes rotational movements. Therefore, any artificial joint, in order to offer the best possible functionality and greater survivability, should also allow rotational movement. Restrictive designs did not allow this movement, resulting in early relaxation. However, such restrictive designs are still used today, especially for revision interventions.
Photo 1: Revision of total knee arthroplasty with “connected” type arthroplasty

Modern designs of total knee arthroplasty implants
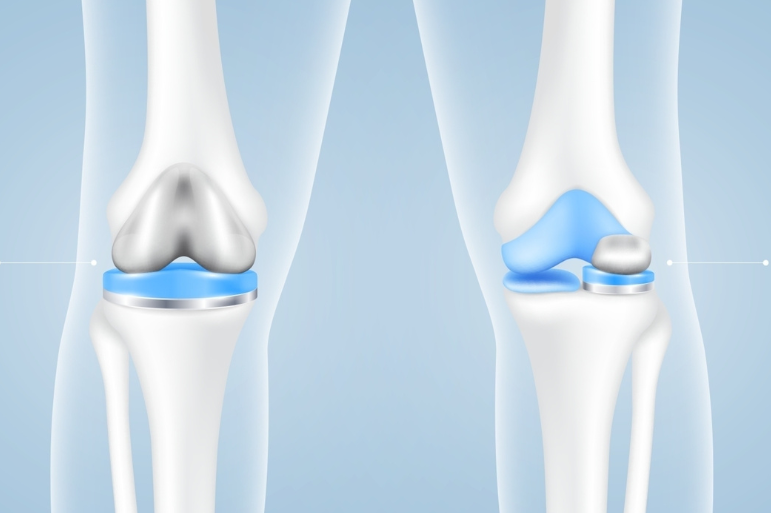
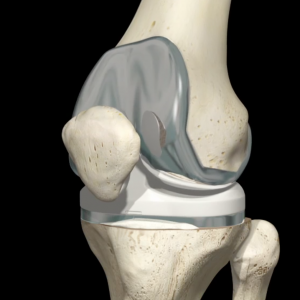
In the early 1970s, a knee arthroplasty design known as “total tuber implantation” was introduced. This involved placing a metal cover around the lower part of the femur and a plastic surface on the upper part of the tibia. The plastic surface was shaped to mimic the normal articular surface of the tibia to allow the joint to flex, extend and twist.
The preservation of the cruciate ligaments, especially the posterior cruciate ligament, during knee replacement, has also been an important parameter in the design of surgery for many years. A number of models of total knee arthroplasty also left the anterior cruciate ligament intact, but they are no longer widely used.
About removing the posterior cruciate ligament is not as bad as it sounds. More specifically, a total knee replacement without cruciate ligaments is better than an arthritic knee with cruciate ligaments. Artificial implants are designed to take into account the lack of cruciate ligaments and compensate for it. For this reason, the plastic tibia implant has a special protrusion that mimics the function of the posterior cruciate ligament, enhancing the stability of the joint.
Nowadays, the replacement or not of the posterior cruciate ligament is a conflicting issue among orthopedists. There are schools that replace the posterior cruciate ligament and those that maintain it. Every school has its arguments.
Photo 2: Total knee arthroplasty
Methods of fixing implants in knee arthroplasty
The “total tuber implant” or “surface knee arthroplasty” is now the benchmark for total knee arthroplasties worldwide.
As with total hip arthroplasty, total knee arthroplasty can be cement-placed or non-cement-based. This terminology refers to the way of fixation needed to connect the artificial prosthesis to the bone.
More specifically, cement fixation involves the use of bone cement (polymethylethacrylate, polymethylmethacrylate) allowing an immediate stable adhesion to the patient’s bone. A cement-free prosthesis needs a coating with a special configuration or coating (for example porous metal or hydroxyapatite) in order to stabilize in the patient’s bone. The goal in both cases is integration, so as to achieve a stable fixation.
The theoretical advantage of a cement-free design is that it makes the revision operation easier if ever needed. It is thought that cement-free designs are easier to remove, but in practice this is not always true. Cement-free designs can sometimes be very difficult to remove during a revision. This is especially observed in cases where a very good osseointegration has been performed. In contrast, removing the prosthesis from the cement is a relatively easy process. Fixing the knee joint with cement has better results and is even considered the best option.
Unicompartmental knee arthroplasty
Sometimes surgeons consider the replacement of the entire knee unnecessary. When knee osteoarthritis is limited to a single compartment , such as its inner part, it is not necessary to replace the entire joint. For this reason, unicompartmental (semi-olic) knee arthroplasties have been developed, which aim to replace only the affected part. This involves replacing either the medial or external segment/compartment of the knee, leaving the unaffected segment intact.
Unicompartmental arthroplasty is a good option, provided that the patient who will undergo it is carefully selected. Arthritis should only really be localized to that part of the joint. If the arthritis is more generalized, it is better to have a total arthroplasty than a semi-total arthroplasty.
Patellofemoral joint arthroplasty
Sometimes patients develop arthritis only in the anterior part of the joint, a part called the patellofemoral joint. This can cause severe symptoms. The modern treatment of this problem is the replacement of the patellofemoral joint. During the operation , the articular surface of the patella is replaced with a special prosthesis, as well as the corresponding part of the femur that articulates with it. It should be noted that the replacement of the patellofemoral joint is not a common operation like total knee arthroplasty. In the past, for these cases , they performed removal of the patella, an operation that is no longer performed.
Photo 3: X-ray of the knee with total knee arthroplasty

During total arthroplasty surgery, the replacement of the patella or not is a conflicting issue among orthopedists. Thus, there are two schools, the mainly American school in which the patella is replaced with a plastic one during surgery and the more European, school in which the patella remains intact and is rejuvenated.
Always in such cases of disagreement there is no golden rule but there are advantages and disadvantages in both cases.
In general, we prefer total knee arthroplasty with the use of cement. Also, the replacement of the posterior cruciate ligament, without replacement of the patella. However, our choice is adapted to the patient’s needs arising from his age, activities, etc.
To sum up, the evolution of total knee replacement has contributed to improving artificial joint functionality, strength, and survival, and patient satisfaction. Surgery is currently an effective solution for the treatment of advanced arthritis. As well, it offers pain relief and a significant improvement in mobility.
After surgery, patients can gradually return to daily activities. Finally, the result of the operation is usually very satisfactory, as the knee works better and the pain is significantly reduced.
If knee pain restricts your movement and affects your daily life, it is important to consult a qualified orthopedic surgeon experienced in modern arthroplasty techniques.
Orthopaedic SurgeonAnastasios Lilikakis is the Director of the Third Orthopaedic Clinic of the Athens Euroclinic and the President of the Department of Hip & Knee Reconstructive Surgery of EEHOT.
Contact us and book your appointment to be responsibly informed about the modern treatment of arthritis and the possibilities of total knee arthroplasty, so that you can safely return to your daily activities.
 Hip Osteoarthritis
Hip Osteoarthritis

 +30 210 7292002
+30 210 7292002
 alilikakis@yahoo.com
alilikakis@yahoo.com