Hip Arthroscopy
INTRODUCTION
Hip arthroscopy is a modern minimally invasive surgical technique, through which it is possible to diagnose and treat many hip diseases.
These guidelines aim to provide general information on:
- the most frequent indications of hip arthroscopy;
- preoperative expectations,
- the main risks of the operation,
- the general framework of postoperative rehabilitation.
This content does not cover all possible cases, as each patient has a particular pathology and may undergo a different type of arthroscopic intervention.
Therefore, there may be substantial variations depending on the individual needs and therapeutic requirements of each case.
WHAT IS HIP ARTHROSCOPY?
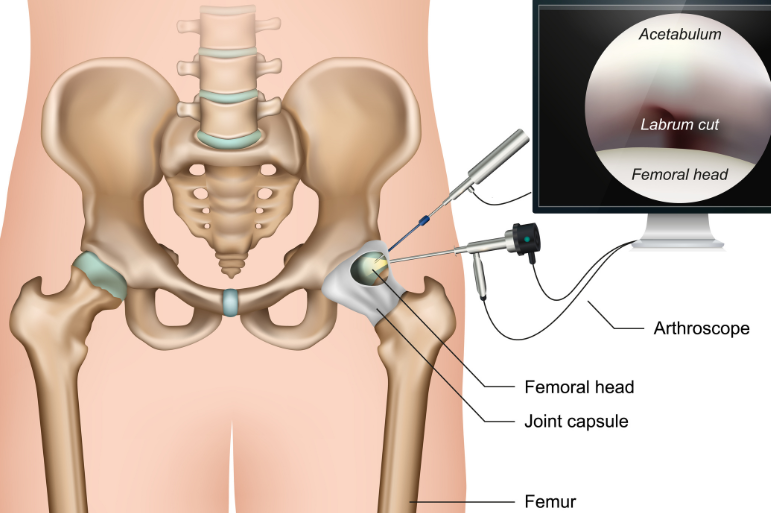
Hip arthroscopy is a minimally invasive surgical technique applied to diagnose and treat hip conditions. It is performed through small incisions, through which a camera and special tools are inserted, allowing direct visual access to the joint and the performance of surgical procedures.
Due to its minimal invasiveness, the advantages of hip arthroscopy are numerous. After surgery, patients are usually mobilized early and gradually return to their daily activities, with clearly improved functionality and quality of life.

HIP ARTHROSCOPY & INDICATIONS
In the early 20th century, hip arthroscopy was considered a technically impossible procedure. But to date, arthroscopy has evolved rapidly. It is a method that is an integral tool of modern reconstructive surgery. With advancements in technology and improved techniques, hip arthroscopy now offers safe and minimally invasive access to the joint.
There are clear and documented indications for which an orthopedic surgeon may recommend arthroscopic hip surgery.
Some of them are the following:
-
- Diagnosis of pain of unknown etiology in the hip joint.
- Removal of free or foreign bodies.
- Correction – debridement of articular cartilage.
- Removal or repair of torn labrum.
- Femoroacetabular impingment correction (FAI).
- Treatment of hip ligament injuries.
- Treating an infection of the hip joint (flushing).
- Treatment of inflammation of the hip joint (synovitis).
- Investigation of painful hip arthroplasty.

WHAT ARE THE TWO MOST COMMON INDICATIONS FOR HIP ARTHROSCOPY?
Probably the two most common indications of hip arthroscopy nowadays are the rupture of the labia cartilage and the symptomatic femorocoilary impact or a combination of these.
More specifically:
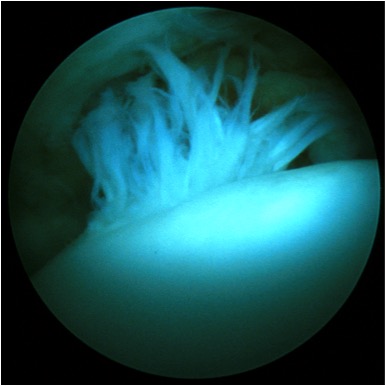
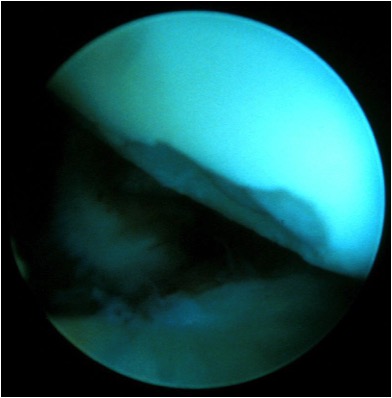
Cartilage labia ruptures
The labrum, which surrounds the acetabulum, can tear or be partially damaged. This is usually associated with femorocoilary impingement, but not always. With hip arthroscopy, the lip cartilage can be cleaned or repaired. Before the operation, MRI, CT and MRI arthrogram of the hip are performed, tests that help a lot in making a diagnosis, but without always making a definitive diagnosis before arthroscopy.
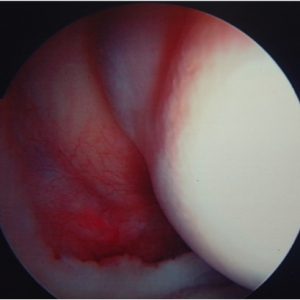
Femoral Impact (FAI)
Femoral impact is a condition that affects the hip joint and is characterized by abnormal contact between the femoral head and the edge of the acetabulum.
This condition leads to damage to the articular cartilage of the acetabulum, the head or both. The labial cartilage is a ring of fibrocartilage tissue, which surrounds the acetabulum and is very similar to the meniscus in the knee, but without performing the same function. A lesion of the labial cartilage will most likely cause pain. An abnormality in the shape of the femoral head or acetabulum, or both, can cause a femoral impact. Activities that involve repetitive, wide-range, hip movement can increase the frequency of this abnormal contact, e.g., sports with high kicks.
Femoral acetabular impingement presents in three forms:
- Cam FAI: The femoral head (or its neck) is not completely spherical, resulting in the formation of a bony lump that bumps into the edge of the acetabulum. Thus, damage is caused to the articular cartilage.
- Pincer FAI: Development of a bony protrusion on the anterior or upper edge of the acetabulum.
- Mixed type FAI: This is a combination of the two previous forms, with simultaneous deformity in the femoral head and acetabulum.
It may affect all age groups and is increasingly recognized as one of the reasons that predispose to hip osteoarthritis. Although the scientific evidence is not yet sufficient, it is believed by many that without early surgical intervention there is a high probability of developing osteoarthritis, resulting in the need for joint replacement (total hip arthroplasty).
Hip arthroscopy can be used to reshape – reshape the femoral head and acetabulum to avoid impact and protect the hip from developing osteoarthritis – at the same time relieving symptoms.
LENGTH OF HOSPITAL STAY AFTER HIP ARTHROSCOPY
The length of the patient’s stay in the hospital after arthroscopy is usually a few hours but will depend on:
- the complexity of the surgery.
- the general state of health of the patient, etc.
ANESTHESIA
Surgery is usually performed under general anesthesia, but not always. If general anesthesia is given, it can also be supplemented with regional anesthesia.
HOW DO WE DO A HIP ARTHROSCOPY?
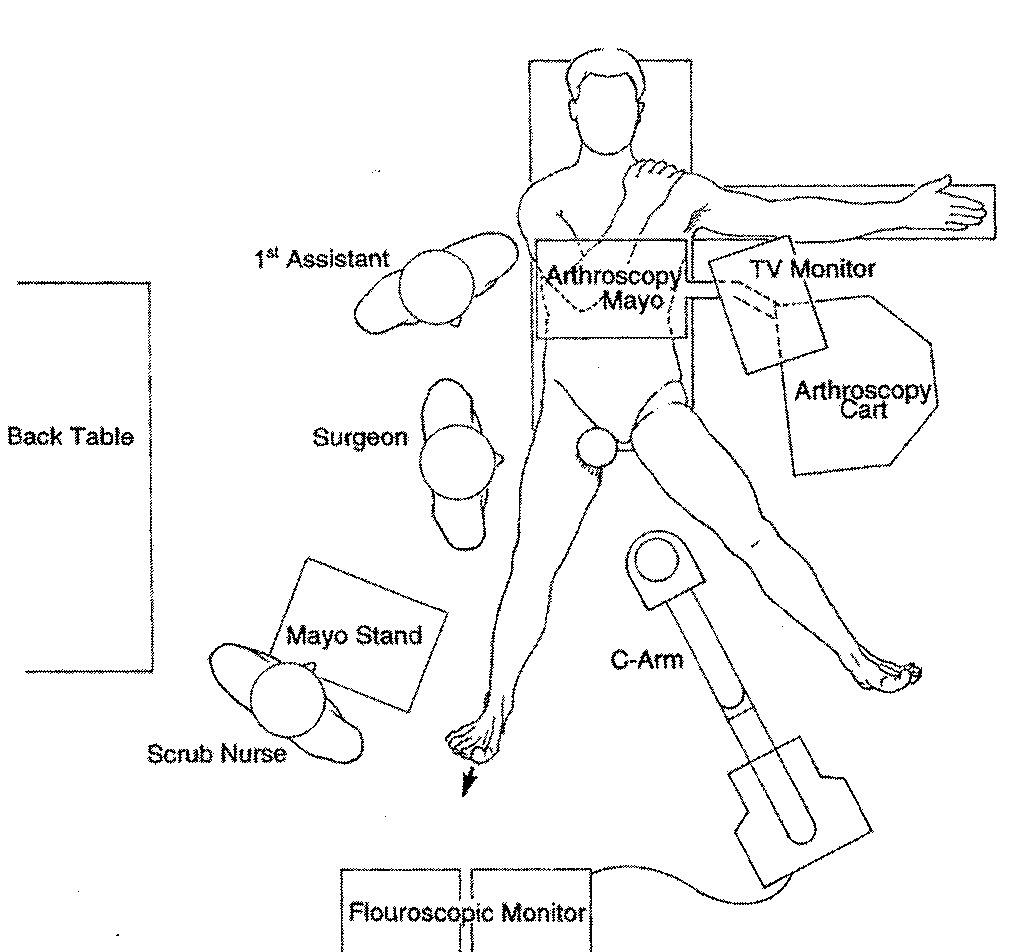
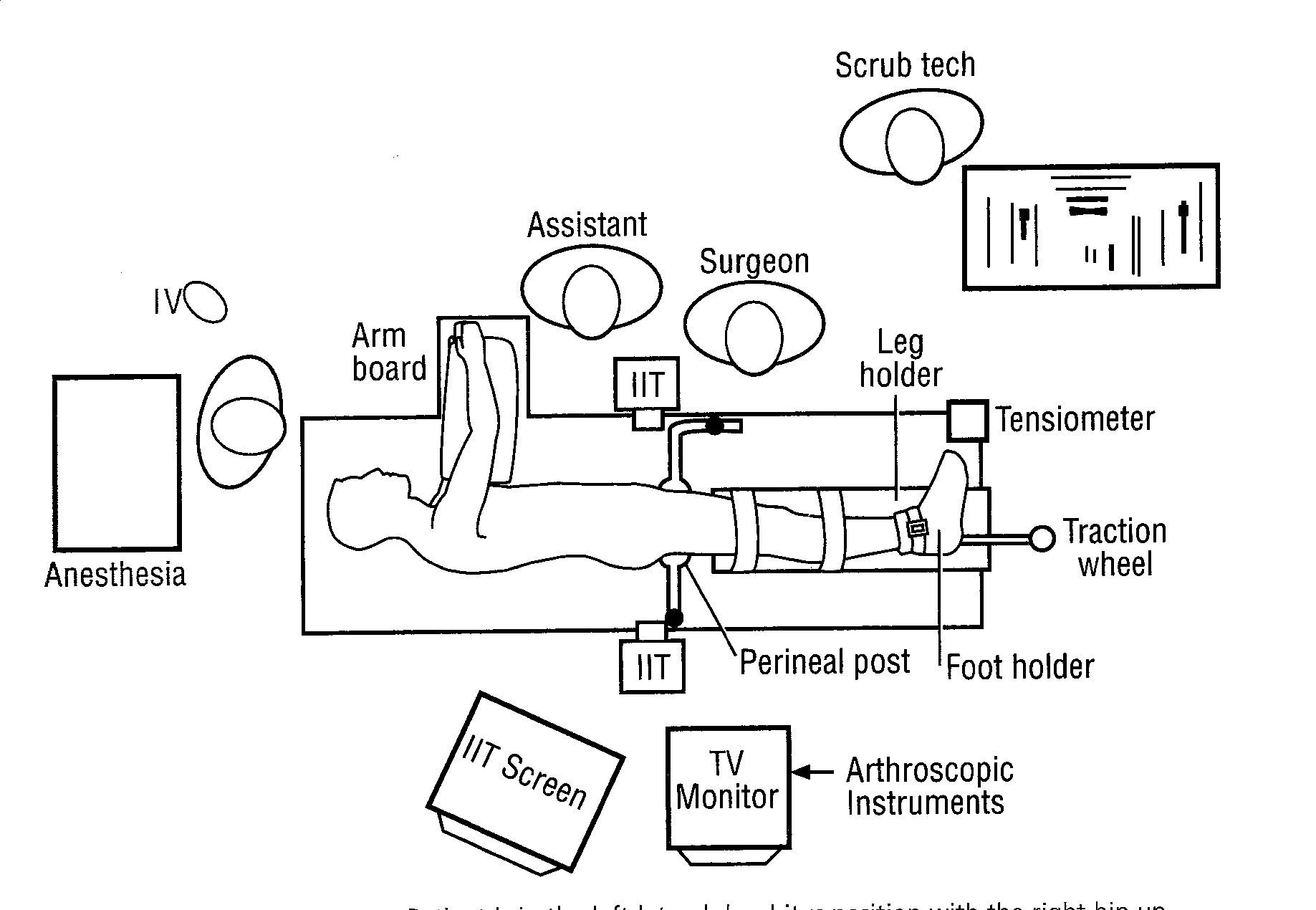
Arthroscopy of the hip in a supine or lateral position
- The bones of the hip joint are removed about a centimeter (the head of the femur from the acetabulum), exerting traction on the leg through a special boot worn by the patient. By “opening” the hip, space is given for the arthroscopy to enter the joint. First, air and/or fluid are injected into the joint under fluoroscopic guidance. After the correct placement of the tools is confirmed, two, three or even four small incisions are made on the side of the hip. Each of these incisions is 5 to 10 millimeters long.
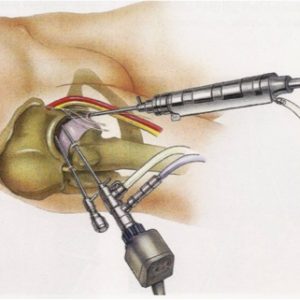
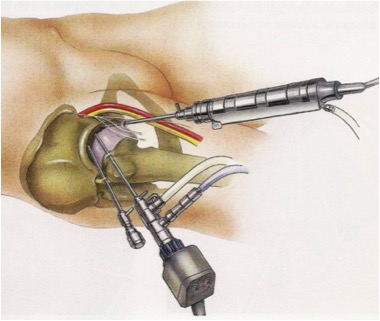
- From these small holes, the arthroscope and arthroscopic instruments enter the joint. The surgeon will thus be able to see inside the joint, identify the problem and proceed accordingly. Very rarely it is not possible for an arthroscope to enter the hip. The duration of the operation varies depending on the problem. Therefore, it can take anywhere from 30 minutes to 120 minutes or even more. During the operation, the use of fluoroscopy can help orient the surgeon on the hip.
- At the end of the operation, drugs are injected into the joint to minimize postoperative pain.
- Small holes are closed with 1-2 stitches or adhesive tapes, while an additional coating is placed on top.
 AFTER HIP ARTHROSCOPY
AFTER HIP ARTHROSCOPY
- Usually the patient feels a discomfort in the hip after the operation. This discomfort can extend to the waist, buttocks, knee and ankle. In any case, it is effectively treated with the appropriate analgesic treatment. In the majority of cases there will be swelling in the groin, buttocks and thighs. This swelling comes from the fluid used in the operation and subsides in the following days.
- It is very likely that you will be seen by a physiotherapist after the operation. He will guide you in terms of moving with or without bacteria, depending on the surgeon’s instructions. In some cases you may be asked to limit the load you put on the operated leg, while in others you will be able to fully charge. Therefore, you may need bacteria after the operation, for a few days or weeks, depending on the operation you underwent. The surgeon will judge when to stop using the bacteria.
- Observe the wound for possible signs of inflammation (increased tenderness, redness, or swelling). Surgical incisions may show little discharge of blood or sero-bloody fluid for a few days after surgery, which is normal.
- After arthroscopy, a reassessment should be made by the surgeon. It is necessary to review the surgical incisions, remove the sutures and have an extensive discussion of the findings of arthroscopy and surgery. It is a good opportunity for any questions and queries, while the next re-evaluations/meetings will be scheduled depending on the surgery performed.
- The surgeon in collaboration with the physiotherapist will formulate a recovery program suitable for you. After the operation, they will guide you in your return to sports activities depending on your progress, which varies greatly from person to person. Rehabilitation depends both on the condition and the surgical findings, as well as on the duration of the discomfort before the operation.

WALKING AND ACTIVITIES AFTER HIP ARTHROSCOPY
- In the majority of cases, in the eight [8] weeks after the operation, you will be able to walk relatively painlessly and without support. Usually at this point in time you can start running, if you wish. However, you should keep in mind that it may take a period of three to six (3 -6) months (or more) to return to a high/professional level of sports. Any unexpected increase in pain can be treated with ice and anti-inflammatory treatment. The key strategy of recovery/recovery is to regain early range of motion and stability, followed by muscle strength and endurance. Returning to work will depend on the pain and nature of your work.
- There are some activities that require attention or should be avoided until eight [8] weeks after arthroscopy.
In particular, these activities are the following:
-
- Prolonged standing, especially on hard surfaces
- Long-distance walking
- Weight lifting
- Deep squat, bend over and squat
- Sleeping on the side. Try to sleep on your back. If you have to sleep on your side, sleep on the unoperated hip with a pillow under the operated leg, to keep it at torso level.
- Using a clutch in non-manual cars can cause symptoms to flare up in the first couple of weeks and is best avoided.
- The sitting position with hip flexion at 90 degrees. A more blunt angle (e.g. 120 degrees) is suggested. The backrests of the seats in the car can be tilted backwards, for example.
The above suggestions are only indicative. The surgeon and/or physiotherapist may indicate additional positions – movements to avoid.
POTENTIAL RISKS AND COMPLICATIONS OF HIP ARTHROSCOPY
All surgeries carry risks, although every effort is made to minimize them. Complications can be temporary or permanent. Fortunately, permanent complications from hip arthroscopy are rare, and in the majority they are temporary. There are, however, risks that include the general risks of general anesthesia and specific risks of hip arthroscopy.
Complications have been reported to occur in 5% of patients and are most commonly associated with transient numbness/altered sensation in the groin and genitals.
The cause is a combination of hip joint stretching and groin pressure during surgery. Although there is a theoretical risk that the numbness will be permanent, in the majority it completely resolves within a few days.
Other complications include:
- Ulcers and pustules
- Infection
- Hip fracture
- Worsening of pain
- Bleeding
- Nerve paresis
- Abandonment of the operation
- Deep vein thrombosis
- Tool breakage
- Serum extravasation
- Delayed wound healing.
However, many of these complications are extremely rare. For example, the exact rate of infection after hip arthroscopy is unknown, but it is definitely significantly less than 1 in 1000.
If you experience symptoms that indicate hip pathology and are considering arthroscopy, trust a physician with many years of experience and a leading role in the field of hip reconstructive surgery. Orthopaedic Surgeon Anastasios Lilikakis is the Director of the Third Orthopaedic Clinic of the Athens Euroclinic and the President of the Department of Hip & Knee Reconstructive Surgery of EEHOT. Contact us and book your appointment.
 Hip Osteoarthritis
Hip Osteoarthritis

 +30 210 7292002
+30 210 7292002
 alilikakis@yahoo.com
alilikakis@yahoo.com